
In part 1 of this breakdown of the fraud that is the Ebola “virus,” I looked at the three main publications from three different teams of researchers which were submitted to The Lancet in 1977 as proof for the existence of a new “virus” causing haemorrhagic fever in 1976. The three teams, including one based at the CDC in Atlanta, coordinated with the WHO in order to associate the new “virus” with the non-specific symptoms of disease occuring in Zaire. They did so even though every piece of information aquired through their investigations pointed to the Marburg “virus,” which itself was based on the acquisition of fraudulent indirect evidence in 1967.
As the WHO was intimately involved in the coordination of these three teams and the determination of the Ebola “virus” as the causative agent, I thought it would be fun to go through their own recounting of the events that led to this conclusion. In 1978, the WHO was kind enough to release a 23-page report that served as a summary of the information that was aquired during the investigation into the outbreak of haemorrhagic fever in a hospital in Zaire. As the report is rather long, I will provide the relevant highlights. In order to make it easier to breakdown and emphasize the pertinent information, I am doing things a little differently this time around. Instead of presenting the highlights as one continuous text, the provided sections from the report will be broken up by commentary with additional information inserted along the way. There is still the usual summary at the end as well as a link to download the entire report for anyone to read if they so desire. So with that being said, let’s jump in and see what we can uncover about this “virus” directly from the WHO:
Ebola haemorrhagic fever in Zaire, 1976
“Between 1 September and 24 October 1976, 318 cases of acute viral haemorrhagic fever occurred in northern Zaire. The outbreak was centred in the Bumba Zone of the Equateur Region and most of the cases were recorded within a radius of 70 km of Yambuku, although a few patients sought medical attention in Bumba, Abumombazi, and the capital
city of Kinshasa, where individual secondary and tertiary cases occurred. There were 280 deaths, and only 38 serologically confirmed survivors.
I want to start by immediately pointing out in this following section, we will see that the common denominator seen in the vast majority of these cases of haemorrhagic fever was the injection of drugs like chloroquine, an anti-malaria drug, at a hospital in Zaire. While I will discuss the use of chloroquine a little later, note that the initial patient was given this injection as he was presumed to have malaria based on his symptoms. After the injection, his symptoms went into clinical remission yet he once again came down with a fever 5 days after his treatment. Spoiler alert: we will later find out that the patient experienced gastrointestinal bleeding after receiving chloroquine and ultimately died on September 8th, 1976:
The index case in this outbreak had onset of symptoms on 1 September 1976, five days after receiving an injection of chloroquine for presumptive malaria at the outpatient clinic at Yambuku Mission Hospital (YMH). He had a clinical remission of his malaria symptoms. Within one week several other persons who had received injections at YMH also suffered from Ebola haemorrhagic fever, and almost all subsequent cases had either received injections at the hospital or had had close contact with another case. Most of these occurred during the first four weeks of the epidemic, after which time the hospital was closed, 11 of the 17 staff members having died of the disease. All ages and both sexes were affected, but women 15-29 years of age had the highest incidence of disease, a phenomenon strongly related to attendance at prenatal and outpatient clinics at the hospital where they received injections. The overall secondary attack rate was about 5%, although it ranged to 20% among close relatives such as spouses, parent or child, and brother or sister.
Note above that pregnant women were among the highest incidence of the symptoms of disease said to be Ebola. Remember this piece of information from the WHO in part 1?
“It can be difficult to clinically distinguish EVD from other infectious diseases such as malaria, typhoid fever and meningitis. Many symptoms of pregnancy and Ebola disease are also quite similar.”

According to the WHO, pregnancy symptoms mimic Ebola. Strangely enough, pregnant women seemingly had the highest incidence of the disease in 1976 and were given injections (presumably of chloroquine but this is not directly stated) in the prenatal and outpatient clinics. What a coincidence!
Active surveillance disclosed that cases occurred in 55 of some 550 villages which were examined house-by-house. The disease was hitherto unknown to the people of the affected region. Intensive search for cases in the area of north-eastern Zaire between the Bumba Zone and the Sudan frontier near Nzara and Maridi failed to detect definite evidence of a link between an epidemic of the disease in that country and the outbreak near Bumba. Nevertheless it was established that people can and do make the trip between Nzara and Bumba in not more than four days: thus it was regarded as quite possible that an infected person had travelled from Sudan to Yambuku and transferred the virus to a needle of the hospital while receiving an injection at the outpatient clinic.
In this next section, the WHO points out that the symptoms of Ebola are non-specific. They tried to add other conditions under the Ebola brand such as hepatitis, pancreatitis, and disseminated intravascular coagulation (a blood clotting condition leading to massive bleeding associated with inflammation, infection, and cancer) yet the lab results were inconlusive:
Both the incubation period, and the duration of the clinical disease averaged about one week. After 3-4 days of non-specific symptoms and signs, patients typically experienced progressively severe sore throat, developed a maculopapular rash, had intractable abdominal pain, and began to bleed from multiple sites, principally the gastrointestinal tract. Although laboratory determinations were limited and not conclusive, it was concluded that pathogenesis of the disease included non-icteric hepatitis and possibly acute pancreatitis as well as disseminated intravascular coagulation.
As I showed in part 1, the particles claimed to be the Ebola “virus” were admitted to be morphologically identical to those associated with the Marburg “virus” yet the WHO and their counterparts at the CDC stated that these “viruses” were immunologically different based on non-specific indirect antibody results. Interestingly, the “virus” was only said to be “isolated” in 8 of 10 cell cultures performed and the particles were only said to be found in the liver samples of three cases:
This syndrome was caused by a virus morphologically similar to Marburg virus, but immunologically distinct. It was named Ebola virus. The agent was isolated from the blood of 8 of 10 suspected cases using Vero cell cultures. Titrations of serial specimens obtained from one patient disclosed persistent viraemia of 10^6.5-10^4.5 infectious units from the third day of illness until death on the eighth day. Ebola virus particles were found in formalin fixed liver specimens from three cases. Survivors of infection were found to have indirect fluorescent antibodies to Ebola virus in titres of 1:64-1:256 within three weeks after onset of disease and these serum titres persisted with only slight decrease for a period of 4 months.
A total of 201 units (200-300 ml each) of plasma containing Ebola virus antibodies in titres of at least 1:64 were obtained and frozen. Two of these units were used to treat a laboratory worker infected with Ebola virus. This person recovered, which suggests that the antibodies may have helped therapeutically.
Note in this next section, the WHO admits that the transmission of the “virus” ended when stopping the injections at the hospital. How odd. 🤔
Virus transmission was interrupted by stopping injections and by isolation of patients in their villages. Use of protective clothing and respirators, strict isolation of patients, and careful disposal of potentially contaminated excreta and fomites will almost certainly prevent future major outbreaks. The virus is probably rarely transmitted by intfectious aerosols, although infection via large droplets remains a possibility.
We also learn that Ebola antibodies were found in five people who were never sick and had no history of contact with any infected individuals. What this ultimately means is that the WHO was strategically setting the stage so that they have the excuse ready for asymptomatic cases of Ebola when the so-called “specific” antibodies are found in people that they are not supposed to be found in:
Only limited ecological investigations were made, since the epidemiology of the outbreak strongly suggested that the virus had been imported into Bumba Zone. Ebola virus was not
recovered from representative samples of bedbugs or of rodents (Rattus rattus and Mastomys spp.) having more or less close contact with humans. Ebola virus antibodies were found, however, in five persons who were not ill and had not had contact with the “infected” villages or the Yambuku hospital during the epidemic. If these findings can be confirmed by an independent method of testing, they would suggest that the virus is in fact endemic to the region and should lead to further effort to uncover a viral reservoir in Zaire.”
If we are to believe the findings as presented by the WHO, the Ebola “virus” originated from an infected person traveling from Sudan to Zaire. This unidentified person recieved treatment at the Yambuku hospital by way of a parenteral injection. The same needle was not sterilized and was then reused on another unsuspecting patient, thus resulting in the spread of the disease from patient-to-patient by way of the continuous use of the same unsterlized needles.

In this next section, the WHO plants the seed for the narrative to follow. It is claimed that only 5 syringes and needles were used for every patient throughout the day. While the WHO claims the needles were not sterilized, they state that the needles were rinsed in pans of warm water and/or boiled.
“Five syringes and needles were issued to the nursing staff each morning for use at the outpatient department, the prenatal clinic, and the impatient wards. These syringes and needles were apparently not sterilized between their use on different patients but rinsed in a pan of warm water. At the end of the day they were sometimes boiled. The surgical theatre had its own ample supply of instruments, syringes, and needles, which were kept separately and auto-claved after use.
Contrary to what the WHO says, the use of heat is a common form of sterilization in hospitals:
“Sterilization is the process of killing harmful microorganisms and bacteria on an object by subjecting them to an environment that they can’t endure.
Sterilization can be performed via two main routes: heat application and chemical means.
Heat is the most common form of sterilization and is used in most hospitals and doctors’ offices via an autoclave.”
https://study.com/academy/lesson/how-to-sterilize-a-needle.html
The WHO also states that the surgery department used syringes and needles that are autoclaved after use. Thus, we are supposed to believe that the hospital in Zaire apparently had different protocols for sterilizing syringes/needles between outpatient, inpatient, and the prenatal ward versus the surgery department. While possible, is it likely? Does it even matter? As we learned earlier, the WHO stated that “viral” transmission stopped as injections at the hospital stopped. They did not say injections using unsterilized needles. What the WHO wants us to believe is that the “virus” transmission stopped due to the “virus” not being transferred by injections using unsterilized needles being passed between the patients. However, as is always the case, there is a much more plausible and likely scenario.

The index patient was injected with chloroquine after being diagnosed with malaria. In fact, his gastrointestinal bleeding did not occur until after the use of chloroquine. This anti-malaria drug is a well-known for its toxic and serious side effects. For a full listing of the reported side effects you can click here but I want to highlight a few of the relevant ones:
- back, leg, or stomach pains
- black, tarry stools
- blood in the urine or stools
- fever
- skin rash, hives, or itching
- sore throat
- unusual bleeding or bruising
- upper right abdominal or stomach pain
- vomiting
Now reread this section from earlier in the WHO’s report:
“After 3-4 days of non-specific symptoms and signs, patients typically experienced progressively severe sore throat, developed a maculopapular rash, had intractable abdominal pain, and began to bleed from multiple sites, principally the gastrointestinal tract.”
Looks like the symptoms for severe Ebola line up perfectly with the side effects from chloroquine injection. Go figure. 🤷♂️
Interestingly, chloroquine has been studied as a drug to treat Ebola patients yet in animals models, it led to worsening of the conditions and death:
“However, while chloroquine inhibited Ebola virus replication in vitro, it caused rapid worsening of Ebola infection in guinea pigs and made no difference to mortality in mice or hamsters.”
More about chloroquine and hydroxychloroquine
“When the same dose (90 mg/kg) of chloroquine was given to hamsters challenged with MA EBOV, the study had to be terminated on day 2 after treatment. Nearly all the treated animals, in both the MA EBOV and the mock-challenged groups, died of acute toxicity after administration of chloroquine intraperitoneally, typically within 30 min after treatment (Figure 2, panel B).”
https://wwwnc.cdc.gov/eid/article/21/6/15-0176_article
Thus, we must ask ourselves what makes more sense logically. Was it the “unsterlized” needles spreading a new “virus” or the side effects of injections of toxic drugs which resulted in the symptoms claimed to be Ebola?

The following section below details what a probable, possible, and proven case of Ebola is. According to the WHO:
- Probable: living in endemic area, had received an injection or been around a probable or proven case and died after experiencing 2 or more symptoms
- Proven: the “virus” was either “isolated” or demonstrated by electron microscopy or they had antibody titres within three weeks of symptoms
- Possible: a person with a headache or fever with or without other symptoms who had contact with a probable or proven case
Interestingly, the WHO notes that possible cases were treated with antimalarial drugs, antibiotics, and antipyretics to exclude other diseases common to the area. In other words, if they weren’t a probable/proven case before treatment, they most likely were afterwards:
“A probable case of Ebola haemorrhagic fever was a person living in the epidemic area who died after one or more days with two or more of the following symptoms and signs: headache, fever, abdominal pain, nausea and/or vomiting, and bleeding. The patient must have, within the three preceding weeks, received an injection or had contact with a probable or a proven case, the illness not having been otherwise diagnosed on clinical grounds. A proven case was a person from whom Ebola virus was isolated or demonstrated by electron microscopy or who had an indirect fluorescent antibody (IFA) titre of at least 1:64 to Ebola virus within three weeks after onset of symptoms. An Ebola virus infection was deemed to have occurred in persons who had a similar IFA antibody titre, but had not been ill during the period 30 August to 15 November 1976.
A possible case was a person with headache and/or fever for at least 24 hours, with or without other signs and symptoms, who had contact with a probable or a proven case within the previous three weeks. These patients were treated with antimalarial drugs, antibiotics, and antipyretics to exclude other diseases common to the area. Persons reporting such symptoms retrospectively were bled and their sera were tested for Ebola virus antibodies. Also any case of fever with bleeding reported to the Ministry of Health from any part of Zaire, whatever the clinical outcome, was regarded as a possible case, and every effort was made to establish a diagnosis by virological or histopathological means.”

What is interesting about this next section is how the surveillance teams set out to find cases of the new disease and how they apparently educated the villagers about a disease that they were supposedly still trying to study and understand themselves. The teams were said to have been educated on the differential diagnosis of Ebola from other diseases:
“The objectives of surveillance teams were to find past and active cases of Ebola haemorrhagic fever, to detect possible convalescent cases, to educate the public as to the nature of and means of preventing the disease, and to establish beyond question the termination of the outbreak. Ten special active surveillance teams were recruited and trained. Each consisted of four persons; a team leader (physician or nurse), two nurses, and a chauffeur. The subjects covered during training were the differential diagnosis of Ebola haemorrhagic fever, its epidemiology (including possible modes of transmission), the means of protecting personnel, and methods for obtaining family census data and recording probable and possible cases. The teams were provided with standard forms, a written schedule, and detailed maps showing the villages they were to cover during a two-week period. Each team was assigned a four-wheel-drive vehicle, some of which had radios, and was provided with food, water, gowns, caps, gloves, boots, respirators, and equipment for obtaining blood samples. Chloroquine, tetracycline, aspirin, and a drug against intestinal parasites were all supplied in tablet form. A physician supervised five teams by frequent field visits and administrative reviews.”
According to the Medical Dictionary, differential diagnosis is defined as:
1. A list of conditions that may cause a particular clinical sign or symptom.
2. The arrival at a diagnosis by means of comparing the similarities and differences in various clinical signs.
https://medical-dictionary.thefreedictionary.com/differential+diagnosis

In order to diagnose a condition, there must be differences in the clinical signs and symptoms. This creates a bit of a problem as the symptoms of Ebola mimic many other more common diseases including influenza, malaria, typhoid fever, meningitis, yellow fever, and even pregnancy. There are no obvious differences in symptomology which is why the CDC and the WHO both state that diagnosis based on symptoms alone is difficult (i.e. impossible) and requires indirect laboratory methods to confirm infection. The CDC states that diagnosis of Ebola requires use of PCR in order to “confirm” a case which was not available to researchers in 1976 as PCR was not invented until 1983. In the WHO’s August 2014 Ebola and Marburg virus disease epidemics: preparedness, alert, control, and evaluation, it is stated that cases must be laboratory confirmed, reiterating that it is done either by way of PCR or by non-specific IgM antibody tests:
“LABORATORY-CONFIRMED CASES:
Any suspected or probable cases with a positive laboratory result. Laboratory-confirmed cases must test positive for the virus antigen, either by detection of virus RNA by reverse transcriptase-polymerase chain
reaction (RT-PCR), or by detection of IgM antibodies directed against Marburg or Ebola.”
There is absolutely no way any of these teams would have been able to differentially diagnose anyone based on clinical symptoms alone. In fact, the researchers in 1976 had 15 possible cases of haemorrhagic fever that mimicked Ebola:
“Fifteen possible cases of haemorrhagic fever occurring outside the main epidemic area were investigated from Kinshasa. Ebola haemorrhagic fever was ruled out in each instance on clinical, virological, or pathological grounds. Final diagnoses included typhoid fever, viral hepatitis, amoebiasis, acute pulmonary oedema, and carbon monoxide poisoning.”
They ultimately decided these 15 cases of haemorrhagic fever were not real cases of Ebola as the results of previously established indirect methods led to diagnoses such as typhoid fever, “viral” hepatitis, amoebiasis, acute pulmonary oedema, and carbon monoxide poisoning. The only method to “diagnose” an Ebola case was either through elimination based on these previously established indirect methods for other diseases associated with the same symptoms or by way of non-specific indirect antibody results. This was the circular way in which they can claim a person experiencing a set of symptoms is an Ebola patient in one case while someone else with the same symptoms is a malaria patient in the other. They love to ignore the fact that, in order for any of these tests to be accurate, not only must the “virus” in question be purified and isolated first in order to calibrate and validate the tests, disease prevalence must also be known first. Disease prevalence can only be determined by clinical diagnosis through differentiating symptoms between these diseases which is an admitted impossibility, thus the case results in 1976 on up to today are utterly meaningless.
Origin and course of the epidemic

As I previously spoiled, we find out here that the initial Ebola patient was diagnosed with malaria, given a chloroquine injection, and had his symptoms subside for a few days only to have them come back worse than before. The patient ultimately died of gastrointestinal bleeding a few days later:
“The first known case, a 44-year-old male instructor at the Mission School, presented himself to the outpatient clinic at Yambuku Mission Hospital (YMH) on 26 August 1976 with a febrile illness thought to be malaria. This man had toured the Mobaye-Bongo zone in the northern Equateur Region by automobile from 10 to 22 August with 6 other Mission workers. The group visited some of the larger towns (Abumombazi, Yakoma, Katokoli, Wapinda) along the road from Yambuku to Badolit, but never arrived at that village because a bridge had been washed away a few kilometres east of the town. On 22 August, fresh and smoked antelope and monkey meat were purchased on the road about 50 km north of Yambuku. The patient and his family ate stewed antelope on his return, but not the monkey meat. He was given chloroquine by parenteral injection on 26 August. His fever resolved rapidly and he was afebrile until 1 September when he again had fever to 39.2° C. Other symptoms and signs ensued and he was admitted to YMH on 5 September with gastrointestinal bleeding. He died on 8 September.
It is also noted that 9 other cases of haemorrhagic fever occurred within the first week and all of them had been treated for other diseases at the hospital. None of the initial diagnoses for these 9 cases were recorded.
At least 9 other cases occurred during the first week of September, all among persons who had received treatment for other diseases at the outpatient clinic at YMH. Names of persons treated at the outpatient clinic and specific diagnoses were not recorded. Thus, it was impossible to determine whether persons with fever had visited YMH in late August. It was of interest, however, that a man about 30 years of age had been admitted to the medical ward on 28 August suffering from “dysentery and epistaxis”, a diagnosis not otherwise listed in the preceding eight months. This man, listed as resident in Yandongi, the capital village of the collectivity some 7 km from Yambuku, was taken from the hospital two days later. He turned out to be a person completely unknown to the residents and authorities of Yandongi.
However, it was stated that parenteral injection was the principal mode of administration of nearly all medicines:
Case histories quickly suggested that YMH was a major source of dissemination of Ebola haemorrhagic fever. It was learned that parenteral injection was the principal mode of administration of nearly all medicines.”
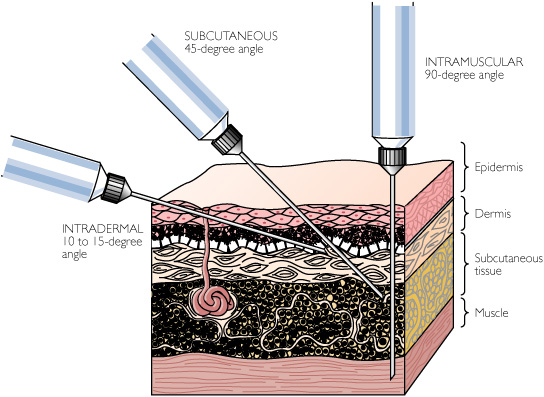
For those unfamiliar, parenteral injections are given through the skin usually in one of five ways: subcutaneous (into the fat), intraperitoneal (in the stomach), intravenous (in the veins), intradermal (under the skin), and intramuscular (in the muscle). This process bypasses the skin and mucuos membranes leading to some notable drawbacks for this mode of treatment such as:
1. Drug administration by these routes is irreversible and poses more risks than the other routes
2. It is an invasive route of drug administration and thus, it can cause fear, pain, tissue damage, and/or infections.
3. Injections have limitations for the delivery of protein products, particularly those that require sustained levels.
4. It is generally riskier.
5. The preparation to be injected has to be sterile.
6. Drug administered by parenteral routes with the exception of intra-arterial route might still be eliminated by first-pass metabolism in liver prior to distribution to the rest of the body.
7. Help is always needed to administer a parenteral dosage form.
https://www.pharmapproach.com/parenteral-route-of-drug-administration-advantages-and-disadvantages/
This affirms that the medical interventions utilizing risky injections with known toxic side effects were the most likely source of disease, including symptoms such as gastrointestinal bleeding. Of course, in the eyes of the WHO, it couldn’t be that the injections of toxic medications were capable of producing said symptoms and were the likely culprit of disease as it had to be a new “virus.” However, how they could possibly conclude this after these next admissions is beyond me:
“All ages and both sexes were affected (Table 3) but females slightly predominated. Age/sex attack rates, using the Yandongi collectivity as the population denominator, showed that adult females had the highest attack rate. Much of this excess illness was associated with receipt of parenteral injections at YMH or one of its clinics. The distribution of disease by age group and type of transmission was essentially equal for both sexes except for injection-associated illness among persons 15-29 years old. Females comprised 22 of 24 such cases in the 21-village study.
The single common risk factor in comparison with matched family and village controls for 85 of 288 cases where the means of transmission was determined, was receipt of one or more injections at YMH. Injections received away from YMH were very unusual. Other factors such as previous case-contact, exposure to food, water, hospital buildings, domestic and wild animals, or travel within three months prior to onset, were not associated with this type of transmission. An additional 149 persons acquired the disease following contact with patients, usually in their home villages, and 43 cases had a history of both patient contact and receipt of injection within three weeks prior to onset of illness. Seventeen persons who lived outside Yambuku had contact at YMH and may have received injections there without reporting this fact to their family.
Most of the cases related to injection occurred during the first 4 weeks of the epidemic (Fig. 4). Indeed, it seems likely that closure of YMH was the
single event of greatest importance in the eventual termination of the outbreak.
Several parameters were compared for persons acquiring infection by contact and injection, respectively. Although no statistically significant differences were found in terms of duration of symptoms and signs of illness (Table 4), no person whose contact was exclusively parenteral injection survived the disease.”
According to the WHO, the excess illness seen was associated with the injections. The disease in women 15-29 years old was higher for those who had been injected during pregnancy. They called these “injection-associated illnesses.” The single common denominator amongst all cases was the receipt of one or more injections of medications capable of producing the symptoms associated with the disease. There were no survivors amongst those who received the injections and after stopping these treatments, the outbreak ended. Even after summarizing these events, the invasive injection and the toxic medications were seemingly not a concern for the WHO. As is always the case, all other much more logical potential causes were pushed aside for the illogical invisible enemy.
“Five consecutive generations of transmission of Ebola haemorrhagic fever were documented in one instance. No sporadic, apparently spontaneous, probable cases were recorded. When “family” was defined as all persons living in contiguous housing and sharing common eating facilities, secondary attack rates never exceeded 8 % (Table 6).”
“In December 1976 and January 1977, sera were solicited from as many people as possible; a total of 236 were obtained. Three persons, 2 of them in clinically noninfected households, who had not had symptoms during or since the epidemic, were found to have Ebola virus IFA titres of at least 1:64. All 3 had experienced contact with fatal cases.”
Serological and ecological studies

In these next few highlights, we find that the antibody measurements, said to be specific and used for diagnosis, are not so specific and were in doubt. The WHO even stated that they were awaiting development of a type-specific method for final interpretation of the antibody results. It is also shown that there were positive antibody reactions found within healthy people who were not recently sick, had no contact with any probable or proven cases, and had no history of visit to the hospital. In other words, the WHO claimed to have found asymptomatic cases of Ebola using antibody tests which they admit produced doubtful results.
“Serum specimens were obtained in November and December 1976 and January 1977 from 984 persons
resident in 48 of the 55 towns and villages reporting probable cases of the disease. These individuals were
classed as clinically ill, not ill but in contact with a case, or neither ill nor in contact. More than half of the subjects were resident in 8 villages, each having more than 5 probable cases. These persons were bled during rapid survey excursions, taking the entire family as the unit of study. The composition of these groups by age, sex, and epidemiological characteristic is given in Table 7 together with the number and category of persons having Ebola virus IFA titres of at least 1:64. Data from Yamolembia I are included. Thirty-eight positives were found. Twenty (16.5%) of 121 ill persons were confirmed as having had Ebola haemorrhagic fever, and 10 (2.5%) of 404 persons in contact with cases also had such antibodies. There were 4 antibody-positive persons who admitted neither illness nor contact with patients. These people were questioned a second time and bled again, and confirmed to have Ebola IFA antibodies. Antibodies were found also in sera of 4 people whose history was not clear and who could not be found a second time for confirmatory study.
In a further effort to document either concurrent asymptomatic infection or possible past infection with Ebola virus, 442 persons were bled in 4 neighbouring villages that had had no fatal cases of the disease. Sera from 5 persons 8-48 years old contained IFA antibodies in titres of 1:64. None of these people were sick, had had contact with persons in other villages, or had visited YMH during the epidemic.
Sera from 58 persons in various exposure categories had anti-Ebola IFA titres of 1:4-1:32. The specificity of these reactions was doubted when it was found that samples from 4 of 200 San Blas Indians from Panama also had such “antibodies” for Ebola but not Marburg virus. Final interpretation of these data awaits development of another method for measurement of type-specific antibodies to these agents.”
The asymptomatic infection excuse is still in use today to cover up finding so-called “specific” antibody results in healthy people. From a 2014 Lancet study:
“Evidence suggests that many Ebola infections are asymptomatic, a factor overlooked by recent outbreak summaries and projections. Particularly, results from one post-Ebola outbreak serosurvey showed that 71% of seropositive individuals did not have the disease; another study reported that 46% of asymptomatic close contacts of patients with Ebola were seropositive.”
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(14)61839-0/fulltext
Hospitalized patients
Here we find that, in 3 cases of EBV at the Ngaliema Hospital, the patients all presented with similar symptoms in the initial stages including fever, headache, anorexia, vomiting, a rash, haemorrhage, and a severe sore throat. However, after a period of days, the symptoms varied between the three patients. This may just have something to do with the fact that each patient was subjected to different toxic treatment cocktails which are outlined in the section below. Not suprisingly, all three succumbed to their ailments after treatment. It was determined that they all suffered hypovolaemic shock, which is a condition where there is sudden and severe blood loss that leads to the heart being unable to pump enough blood throughout the body, eventually resulting in multiple organ failure. One possible cause of this shock is damage to the stomach. What could possibly lead to such an outcome in these patients? Perhaps trauma to the gastrointestinal organs by way of multiple injections of cocktails of toxic medications known to damage the stomach?:
“Early symptoms and signs in all 3 patients at Ngaliema Hospital included fever, headache, anorexia, and vomiting. A morbilliform rash appeared on the anterior trunk in each of these patients on day 5 or 6, spread to the back and limbs, then faded within 48 hours. Haemorrhage and severe sore throat began between the fourth and seventh days of illness.
One patient had oral and conjunctival petechiae beginning on day 4, haematemesis and melaena from day 4, gingival bleeding on day 7, and bleeding from injection sites on day 8. Another had melaena only, beginning on the sixth day of illness. The third patient had a single episode of haematemesis on day 7 followed by melaena and ecchymosis on the next day. Progressive glossitis and pharyngitis beginning on day 3 were noted in one patient who developed severe erythema and oedema of the soft palate and pharynx leading to pronounced dysphagia. All three patients were febrile throughout the course of illness, with temperatures frequently above 39°C. Two patients had terminal tachycardia. One patient died on day 7 and two on the eighth day of illness.
Clinical laboratory tests were done on the first patient, but only a few measurements were carried out on the other two cases to avoid undue exposure of hospital laboratory staff to the virus. Leucocyte counts on the first patient were 7600 and 8900/mm3 on days 5 and 7, respectively. Platelets on days 4, 6, and 7 were 162,000, 150,000 and 150,000/mm3; these were days when frank haemorrhage occurred. During this time, serum SGOT rose from 90 to greater than 200 units/ml and the SGPT increased from 40 to more than 200 units/ml. Serum bilirubin rose from 25.6 tmol/l on day 5 to 59.8 tmol/l on day 7. Partial thromboplastin time (PTT) was 47 seconds on the fifth day. This patient produced only 200 ml of urine on the seventh day and none during the next day when she died. The second patient, on whom no laboratory tests were done, became anuric during the last 2 days of life.
The third patient had white blood cell counts of 9,400 and 12,300/mm3 on days 7 and 8, respectively. Platelet counts on these days were 253,000 and 205,000/mm3, while P17 values were 45 and 50 seconds, respectively. Fibrin degradation products, measured with a commercial kit (Burroughs-Wellcome) were recorded as 1+ and 2+ on days 7 and 8.
The first case was treated with aspirin, antibiotics, corticosteroids, blood transfusion, and intravenous fluids. The second patient received aspirin, hydrocortisone, immunoglobulin, intravenous fluids, and an experimental drug, moroxydine. Enterovioform was given to control diarrhoea but without success. The third patient was treated for unconfirmed malaria during the first 2 days of illness. When the etiological agent of the epidemic was shown to be a Marburg-like virus, she was given, on day 4, 500 ml of Marburg human plasma obtained from a recovered patient in South Africa. This plasma had an IFA titre of 1:32. In anticipation of disseminated intravascular coagulation (DIC), she was given 16,000 units of heparin on day 6 and 30,000 units daily thereafter. Although anticoagulation was unsatisfactory, as shown by the normal PTT on days 7 and 8, she had less clinical bleeding than the other two patients. On the day prior to death she complained of substernal chest pain and had a tachycardia of 136 with a gallop rhythm. Digitalization slowed this rate only slightly. Marked oedema of the face and upper limbs was present.
Although no autopsies were performed, it appeared clinically that these patients died of hypovolaemic shock. Evidence for DIC was fragmentary, but this syndrome may well have precipitated the bleeding and shock in all cases. Postmortem liver biopsy in the first case revealed marked focal hepatic-cell necrosis with large intracytoplasmic eosinophilic inclusions. Marburg virus-like particles were visualized with an electron microscope (2).
Ebola virus was recovered on day 6 from blood specimens from patient 1 and on days 3 and 6 from patient 2. Quantitative virus assays on blood from the third patient are shown in Table 8. No IFA antibodies against Ebola or Marburg viruses were present.
Retrospective field studies

If you needed more reason to doubt antibody results, look no further. In this survey of 231 probable cases, 34 had IFA antibodies. 59% of those with antibodies had symptoms thus leaving 41% of those probable cases asymptomatic. Many others who had direct contact with fatal cases reported having had symptoms but no antibodies whatsoever. In other words, many of those who were sick had no antibodies and nearly half of those who had antibodies were never sick:
Questionnaire forms were completed on 231 probable cases 1 year of age or older, 34 individuals who were found to have Ebola virus IFA antibodies, and 198 controls. The numbers of responses obtained for each symptom and the percentages responding positively in these groups are shown in Table 9. Fever and headache were almost invariably present. The headache often radiated to the cervical spine and was associated with low-back pain radiating into the legs. Sore throat was often reported in association with a sensation of a “ball” in the throat. Chest pain and pleuritis were uncommon. Of persons with antibodies, 59% had one or more symptoms, the most prominent being fever, headache, abdominal pain, and arthralgia. Many more persons who had been in contact with fatal cases reported symptoms but had no Ebola virus antibodies. Illness in antibody-positive individuals was, in general, marked by profound
prostration, weight loss, and a convalescent period of 1-3 weeks.”
According to the WHO, a urinary protein test, one not in use as a diagnostic today, was utilized early on in the outbreak to diagnose cases. How many of these patients were misdiagnosed based on a faulty test?
“The only clinical laboratory test done on patients admitted to Yambuku Hospital was urinary protein. This was reported as uniformly positive and was used as a major diagnostic criterion by the nursing sisters early in the epidemic.
The WHO admits that the virological studies, arguably the most important part of the (pseudo)scientific evidence needed to understand a new “virus,” were limited. This is apparent as they used small sample sizes where “virus isolation” was only attempted in 10 cases and only 4 liver biopsies were performed:
Virological studies were limited. Ebola virus was isolated in African green monkey kidney cells (Vero) from blood specimens in 8 of 10 cases attempted. These specimens were taken 2-13 days after onset of symptoms. Of interest was the simultaneous detection of virus and IFA Ebola antibodies to a titre of 1:32 in one patient. This man was in the 13th and penultimate day of his illness. Ebola virus particles were also visualized in 3 of 4 postmortem liver biopsies obtained from clinically suspect cases.”
The Ebola “virus” was said to have the highest case mortality rate since rabies. Perhaps the toxic cocktails injected into these patients may have helped bring about the high amounts of fatality?:
“No more dramatic or potentially explosive epidemic of a new acute viral disease has occurred in the world in the past 30 years. The case mortality rate of Ebola haemorrhagic fever in Zaire of 88% is the highest on record except for rabies infection. In the circumstances it was not surprising that much desired information was never obtained. Delays in recognition, notification to international health agencies, and specific diagnosis of the disease contributed greatly to this outcome. No better example comes to mind to illustrate the need for national disease surveillance and the prompt solicitation of international assistance, nor of the need for the development of international resources, comprising personnel, equipment, transport, communication, and finance, that can be made available in a very few days to cope with such emergencies.
Interestingly, both Ebola and rabies have a connection to dangerous injections. In the case of rabies, until the 1980’s, the treatment involved a series of shots in the stomach:
“There has been confusion among the general public because of historical fears and the painful
injections of anti-rabies vaccination (nerve tissue vaccine administered over the abdomen) given in the past.”
In fact, there could be as many as 21 injections into the abdomen for rabies:
“Several years ago, treatment for rabies included 21 injections into a person’s stomach. It was extremely painful and involved a long needle. However, since the early 1980s, there’s a much different rabies vaccine to treat humans for rabies exposure.”

As intraperitoneal injections (in the stomach cavity) are one of the 5 routes used for parenteral treatment, could these Ebola patients in 1976 have been given the toxic drugs in this manner as was done for rabies until the 1980’s? Injections of toxic drugs directly into the stomach would be a possible explanation for an increase in gastrointestinal bleeding. Damage to the stomach by way of trauma is also a risk factor for hypovolaemic shock as suffered by the patients in Ngaliema Hospital. Unfotunately, the WHO does not define the route of parenteral injection so we can only speculate.
These next few sections offer some random pieces of information that poke holes into the WHO’s story. First, you will see the WHO admit that laboratory data was virtually non-existent for this outbreak, yet they confirm that the clinical picture resembled the Marburg “virus.” They thought that the agents “isolated” in Sudan and Zaire were identical but they had yet to perform the (previously admitted to be doubtful) antibody testing to confirm this. The WHO claimed that viremia (the presence of “virus” in the blood) is a constant feature of the “virus” based on a single study involving the small sample size of just one patient. However, the WHO then stated that no evidence was obtained for persistent “viral” carriage in the Zaire cases of Ebola infection, a phenomenon documented on two occasions for Marburg “virus,” but warn that this information is based on a small sample size. It seems very clear that the WHO likes to have their cake and eat it too:
Although laboratory data were virtually non-existent, the clinical picture seen in this outbreak resembled illness produced by the related Marburg virus. If anything, the evolution of Ebola haemorrhagic fever appeared to be more inexorable and less variable than Marburg virus infection. Though far from proven, we suspect that acute defibrination syndrome and pancreatitis were major features of the syndrome and severe liver disease was evident.
In contrast to observations made simultaneously in Sudan, the illness in Zaire had fewer respiratory symptoms, a shorter clinical course, and a higher fatality rate (4). Whether this was due to differences in the virulence of the virus per se or to host and ecological variables such as climate (relative humidity) is not known. At the present time the agents recovered from Sudan and Zaire are thought to be identical, although definitive neutralization tests have not yet been done.
Viraemia appears to be a constant feature of Ebola virus infection in man. The virus persisted in large amounts in the blood in the single, well studied case. The finding of both virus and antibodies in the blood of another agonal case 13 days after onset of symptoms raises the possibility, regarded as unlikely, that antigen-antibody complexes may contribute to the pathology of infection. This and a number of other important virological questions can only be pursued for the moment through studies using monkeys. One of the most pressing is the need for a way to make rapid diagnosis in suspected cases of the disease by searching for cells containing viral antigen. Retrospective specific diagnosis of fatal cases by electron microscopic examination of formalin-fixed liver biopsies appears quite promising and should be attempted in all cases of acute febrile haemorrhagic disease in Africa.
No evidence was obtained for persistent viral carriage in the Zaire cases of Ebola infection, a phenomenon documented on two occasions for Marburg virus (5, 6). But it should be remembered that the number of appropriate, immunosequestered sites sampled was very small. However, semen from one patient infected with a Zaire strain of Ebola virus in the United Kingdom contained virus for more than 2 months after onset of symptoms (3).
In the final highlights, we get the WHO’s simplified version of events that reiterates earlier points which should have cast doubt on their conclusions that a new “virus” was the cause of an outbreak of a new disease. First, we get the admittance that the Ebola “virus” had a low rate of secondary person-to-person transmission, meaning it did not easily spread even in cases of close contact with “infected” individuals. They state that the way the new “virus” made it to the hospital will never be known, yet they believed it was brought from the Sudan by man. The way that it was decided that the “virus” spread was through the contaminated needles and syringes used for injections into the sick patients. Once these injections stopped, so too did the outbreak:
The Zaire epidemic had all the attributes of a common source outbreak, together with a fortunately low rate of secondary person-to-person transmission. The means by which the virus was introduced into Yambuku Mission Hospital will probably never be precisely known, but it seems possible that it was brought directly from the Sudan by man. Dissemination of the agent into the villages of the region was principally through contaminated equipment used for parenteral injections. The epidemic waned when the hospital was closed for want of medical staff. That careful disposal of contaminated excreta and fomites, as well as strict barrier nursing using respirators, could break the chain of transmission was demonstrated during the small outbreak in Kinshasa. Still simpler isolation precautions and a change in the cultural customs at funerals appears to have contributed to the dying out of infection in the villages.
Interestingly, the WHO admitted that cases brought about by injection were different and more likely to be fatal than those that they claimed were secondary cases aquired without injections. This obviously makes sense when viewed from the standpoint that the non-specific symptoms of disease were the result of the unnatural injection of various toxic medications directly into the patients and not the effect of a new “virus.” Secondary cases were nothing more than looking for similar symptoms in villagers and using fraudulent antibody results to claim the symptoms were caused by the same imaginary “virus:”
Although the data were not always statistically convincing, we had the strong impression that Ebola haemorrhagic fever acquired by injection differed from that due to contact with another case. The mortality was higher. In one study, secondary transmission rates also were higher from index cases that were parenterally induced. It may be that increased virus replication and excretion following parenteral infection accounts for all or most of these differences, but other causes were by no means excluded.
The WHO went on to admit that “neonatal” cases were not definitively elucidated. In other words, they could not explain how the babies aquired the disease from the mother. There was apparently no questioning of the injections of harmful medications into the pregnant women potentially bringing about death and disease in infants. It had to be this magical “virus” somehow passing through the placenta and infecting the unborn child:
The observed “neonatal” cases of the disease were not definitively elucidated. One wishes to know whether Ebola virus can pass through the placenta and infect the fetus, and whether virus is present in human milk and is infectious if ingested.
Once again hammering the final nail in the coffin of the Ebola “virus,” the WHO reminded us that better antibody tests were needed in order to interpret the results. While fraudulent antibody results should never carry any weight as evidence, these findings were the only way the researchers could differentiate Ebola from “Marburg” and many other “viruses,” thus their questionable “accuracy” speaks volumes. The IFA results were essential to the case that Marburg and Ebola were different “viruses” yet the WHO was unsure if these results were correct. They further add that, like the Marburg “virus,” the source of the Ebola “virus” was unknown. This should tell you everything you need to know:
Finally, a better method for measuring Ebola virus antibodies is needed in order to interpret the serological findings reported here. That less than 20% of persons gave a history of acute illness following contact with a fatal case was no surprise. Most of these persons had mild, self-limiting diseases, these being highly endemic in the area. But if the IFA data are correct, at least 2.5% of persons in contact with fatal cases experienced subclinical infection. In addition, the finding of antibodies in a few individuals in the absence of any known contact with Ebola virus during the epidemic raises the possibility that the agent is in fact endemic in the Yambuku area and is occasionally transmitted to man. A definitive answer is essential to further ecological exploration of what is now a very mysterious agent. As in the case of Marburg virus, the source of Ebola virus is completely unknown beyond the simple fact that it is African in origin.”

In Summary:
- Between September 1st and October 24th, 1976, 318 cases of (assumed) acute “viral” haemorrhagic fever occurred in northern Zaire
- There were 280 deaths, and only 38 serologically confirmed (i.e. non-specific antibody results) survivors
- The index case in this outbreak had onset of symptoms on September 1st, 1976, five days after receiving an injection of chloroquine for presumptive malaria at the outpatient clinic at Yambuku Mission Hospital (YMH).
- He had a clinical remission of his malaria symptoms
- Within one week several other persons who had received injections at YMH also suffered from Ebola haemorrhagic fever, and almost all subsequent cases had either received injections at the hospital or had had close contact with another case
- All ages and both sexes were affected, but women 15-29 years of age had the highest incidence of disease, a phenomenon strongly related to attendance at prenatal and outpatient clinics at the hospital where they received injections
- Intensive search for cases in the area of north-eastern Zaire between the Bumba Zone and the Sudan frontier near Nzara and Maridi failed to detect definite evidence of a link between an epidemic of the disease in that country and the outbreak near Bumba
- Nevertheless it was established that people can and do make the trip between Nzara and Bumba in not more than four days: thus it was regarded as quite possible that an infected person had travelled from Sudan to Yambuku and transferred the “virus” to a needle of the hospital while receiving an injection at the outpatient clinic
- In other words, they could not establish any link between two outbreaks but still assumed it was possible for a hypothetical scenario where an unknown “infected” individual carried a new “virus” and made their way to the hospital and unknowingly transmitted the new “virus” by way of the same needle being used with other patients
- After 3-4 days of non-specific symptoms and signs, patients typically experienced
progressively severe sore throat, developed a maculopapular rash, had intractable abdominal pain, and began to bleed from multiple sites, principally the gastrointestinal tract - Although laboratory determinations were limited and not conclusive, it was concluded that pathogenesis of the disease included non-icteric hepatitis and possibly acute pancreatitis as well as disseminated intravascular coagulation
- This syndrome was caused by a “virus” morphologically similar to Marburg “virus,” but immunologically distinct (i.e. everything was identical besides non-specific antibody results)
- The agent was “isolated” from the blood of 8 of 10 suspected cases using Vero cell cultures
- Ebola “virus” particles were found in formalin fixed liver specimens from three cases
- Survivors of infection were found to have indirect fluorescent antibodies to Ebola “virus”
- A total of 201 units (200-300 ml each) of plasma containing Ebola “virus” antibodies in titres of at least 1:64 were obtained and frozen and used on an “infected” person who recovered, which suggested to them that the antibodies may have helped therapeutically (and the invisible antibodies may have done absolutely nothing while the person recovered despite their use so it amounts to pointless speculation)
- “Virus” transmission was interrupted by stopping injections and by isolation of patients in their villages (i.e. the stoppage of injections of chloroquine ended the “viral” spread… 🤔)
- They somehow decided that the “virus” is probably rarely transmitted by intfectious aerosols, although infection via large droplets remains a possibility (yet more evidenceless and baseless speculation)
- Ebola “virus” antibodies were found in five persons who were not ill and had not had contact with the “infected” villages or the Yambuku hospital during the epidemic (in other words, the antibodies were either non-specific and/or there are asymptomatic Ebola patients walking around…or the more likely scenario that it is all fraudulent)
- Five syringes and needles were issued to the nursing staff each morning for use at the outpatient department, the prenatal clinic, and the impatient wards
- These syringes and needles were apparently not sterilized between their use on different patients but rinsed in a pan of warm water and at the end of the day they were sometimes boiled
- This led the researchers to conclude it was a “virus” being transmitted from person-to-person due to needle use rather than the contents of the injection
- On a side note, chloroquine injections, as was given to the patients, are known to cause the exact same symptoms associated with Ebola:
- back, leg, or stomach pains
- black, tarry stools
- blood in the urine or stools
- fever
- skin rash, hives, or itching
- sore throat
- unusual bleeding or bruising
- upper right abdominal or stomach pain
- vomiting
- A probable case of Ebola haemorrhagic fever was a person living in the epidemic area who died after one or more days with two or more of the following symptoms and signs: headache, fever, abdominal
pain, nausea and/or vomiting, and bleeding- The patient must have, within the three preceding weeks, received an injection or had contact with a probable or a proven case, the illness not having been otherwise diagnosed on clinical grounds
- A proven case was a person from whom Ebola “virus” was “isolated” or demonstrated by electron microscopy or who had an indirect fluorescent antibody (IFA) titre of at least 1:64 to Ebola “virus” within three weeks after onset of symptoms
- An Ebola “virus” infection was deemed to have occurred in persons who had a similar IFA antibody titre, but had not been ill during the period August 30th to November 15th, 1976
- A possible case was a person with headache and/or fever for at least 24 hours, with or without other signs and symptoms, who had contact with a probable or a proven case within the previous three weeks
- These patients were treated with antimalarial drugs, antibiotics, and antipyretics to exclude other diseases common to the area
- In other words, as long as you experienced one or two of the non-specific symptoms and either had an injection or been around those who were deemed probable/proven by way of indirect electron microscopy or non-specific antibody results, you were considered an Ebola patient
- The objectives of surveillance teams were to find past and active cases of Ebola haemorrhagic fever, to detect possible convalescent cases, to educate the public as to the nature of and means of preventing the disease, and to establish beyond question the termination of the outbreak (how did they educate the public on the nature and means of preventing a “virus” they were still supposedly identifying and studying? 🤔)
- The subjects covered during training were the differential diagnosis of Ebola haemorrhagic fever, its epidemiology (including possible modes of transmission), the means of protecting personnel, and methods for obtaining family census data and recording probable and possible cases (how could they differentially diagnose a disease that mimicked many other diseases sharing the exact same symptoms…and even pregnancy?)
- Chloroquine, tetracycline, aspirin, and a drug against intestinal parasites were all supplied in tablet form (because if you can’t find cases naturally, you might as well create them)
- Fifteen possible cases of haemorrhagic fever occurring outside the main epidemic area were investigated from Kinshasa and Ebola haemorrhagic fever was ruled out in each instance on clinical, virological, or pathological grounds (i.e. the indirect evidence pointed to other assumed causes)
- Final diagnoses included:
- Typhoid fever
- “Viral” hepatitis
- Amoebiasis
- Acute pulmonary oedema
- Carbon monoxide poisoning
- The first patient was given chloroquine by parenteral injection on August 26th and his fever resolved rapidly and he was afebrile until 1 September when he again had fever to 39.2° C
- Other symptoms soon followed and he was admitted to YMH on September 5th with gastrointestinal bleeding and died on September 8th
- It was learned that parenteral injection (injections into the body by various routes) was the principal mode of administration of nearly all medicines
- The single common risk factor in comparison with matched family and village controls for 85 of 288 cases where the means of transmission was determined, was receipt of one or more injections at YMH
- Other factors such as previous case-contact, exposure to food, water, hospital buildings, domestic and wild animals, or travel within three months prior to onset, were not associated with this type of transmission
- 43 cases had a history of both patient contact and receipt of injection within three weeks prior to onset of illness
- Seventeen persons who lived outside Yambuku had contact at YMH and may have received injections there without reporting this fact to their family
- No person whose contact was exclusively parenteral injection survived the disease
- Indeed, it seems likely that closure of YMH was the
single event of greatest importance in the eventual termination of the outbreak - In other words, the risky and unnatural mode of injection as well as the toxic medications capable of producing the same exact symptoms are all that is needed to explain these cases, not a new invisible “virus”
- No sporadic, apparently spontaneous, probable cases were recorded
- When “family” was defined as all persons living in contiguous housing and sharing common eating facilities, secondary attack rates never exceeded 8%
- Efforts were made to document either concurrent asymptomatic infection or possible past infection with Ebola “virus”
- Sera from 5 persons 8-48 years old contained IFA antibodies in titres of 1:64 and none of these people were sick, had had contact with persons in other villages, or had visited YMH during the epidemic (i.e. they were asymptomatic)
- Sera from 58 persons in various exposure categories had anti-Ebola IFA titres of 1:4-1:32 yet the specificity of these reactions was doubted when it
was found that samples from 4 of 200 San Blas Indians from Panama also had such “antibodies” for Ebola but not Marburg “virus” - Final interpretation of these data awaited development of another method for measurement of type-specific antibodies to these agents
- In other words, the antibody results claimed to be specific were not so specific and the antibody results needed to be confirmed with a yet undeveloped “more specific” method
- Early symptoms and signs in all 3 patients at Ngaliema Hospital included fever, headache, anorexia, and vomiting yet the remaining symptoms varied amongst them
- Clinical laboratory tests were done on the first patient, but only a few measurements were carried out on the other two cases to avoid undue exposure of hospital laboratory staff to the “virus”
- The first patient was treated with aspirin, antibiotics, corticosteroids, blood transfusion, and intravenous fluids
- The second patient received aspirin, hydrocortisone, immunoglobulin, intravenous fluids, an experimental drug, moroxydin, and enterovioform to control diarrhoea but without success
- The third patient was treated for unconfirmed malaria during the first 2 days of illness and when the etiological agent of the epidemic was shown to be a Marburg-like “virus,” she was given, on day 4, 500 ml of Marburg human plasma obtained from a recovered patient in South Africa
- All three patients died after treatment
- Although no autopsies were performed, it appeared clinically that these patients died of hypovolaemic shock (rapid loss of blood that can be caused by internal bleeding in the abdominal organs and digestive tract)
- Marburg “virus-like” particles were visualized with an electron microscope in one case
- No IFA antibodies against Ebola or Marburg “viruses” were present in any of the 3 victims
- Questionnaire forms were completed on 231 probable cases 1 year of age or older, 34 individuals who were found to have Ebola “virus” IFA antibodies, and 198 controls
- Of persons with antibodies, 59% had one or more symptoms, (41% apparently had no symptoms) the most prominent being fever, headache, abdominal pain, and arthralgia
- Many more persons who had been in contact with fatal cases reported symptoms but had
no Ebola “virus” antibodies - Here we can see how unreliable antibody results are when 41% had no symptoms of disease and those who had symptoms after contact with fatal cases had no antibodies whatsoever
- The only clinical laboratory test done on patients admitted to Yambuku Hospital was urinary protein which was reported as uniformly positive and then used as a major diagnostic criterion by the nursing sisters early in the epidemic (note: this is not a diagnostic used today which leads one to wonder how many early cases were misdiagnosed using a faulty method no longer in use?)
- Virological studies were said to be limited
- Ebola “virus” was “isolated” in African green monkey kidney cells (Vero) from blood specimens in 8 of 10 cases attempted.
- Ebola “virus” particles were also visualized in 3 of 4 postmortem liver biopsies obtained from clinically suspect cases
- The case mortality rate of Ebola haemorrhagic fever in Zaire of 88% is the highest on record except for rabies infection
- Although laboratory data were virtually non-existent, the clinical picture seen in this outbreak resembled illness produced by the related Marburg “virus”
- At that time, the agents recovered from Sudan and Zaire were thought to be identical, although definitive neutralization tests had not yet been done
- Viraemia appeared to be a constant feature of Ebola “virus” infection in man as the “virus” persisted in large amounts in the blood in the single, well studied case (one case 🤣)
- The WHO stated that a number of other important virological questions can only be pursued for the moment through studies using monkeys
- No evidence was obtained for persistent “viral” carriage in the Zaire cases of Ebola infection, a phenomenon documented on two occasions for Marburg “virus”
- The Zaire epidemic had all the attributes of a common source outbreak, together with a fortunately low rate of secondary person-to-person transmission (i.e. not that infectious nor transmissable)
- According to the WHO, the means by which the “virus” was introduced into Yambuku Mission Hospital will probably never be precisely known, but it seemed possible that it was brought directly from the Sudan by man
- Dissemination of the agent into the villages of the region was principally through contaminated equipment used for parenteral injections (see how they made it about “contaminated” needles rather than the mode of injection with numerous toxins?)
- The epidemic waned when
the hospital was closed for want of medical staff (and thus stopping the injections of toxic drugs) - The WHO had the strong impression that Ebola haemorrhagic fever acquired by injection differed from that due to contact with another case as the mortality was higher
- The observed “neonatal” cases of the disease were not definitively elucidated
- The WHO again admitted that a better method for measuring Ebola “virus” antibodies was needed in order to interpret the serological findings reported here (which is a pretty troubling admittance when the only way they claimed a new “virus” as well as past and present cases was based on antibody results)
- That less than 20% of persons gave a history of acute illness following contact with a fatal case was apparently no surprise
- The WHO stated that if the IFA data are correct, at least 2.5% of persons in contact with fatal cases experienced subclinical infection (those antibody results sure seem rather sketchy based on the WHO’s continued hesitancy about their accuracy)
- In addition, the finding of antibodies in a few individuals in the absence of any known contact with Ebola “virus” during the epidemic raised the possibility that the agent is in fact endemic in the Yambuku area and is occasionally transmitted to man
- As in the case of Marburg “virus,” the source of Ebola “virus” is completely unknown beyond the simple fact that it is African in origin

If we are to believe the findings as presented by the WHO, the Ebola “virus” originated from an infected person traveling from Sudan to Zaire. This unidentified person received treatment at the Yambuku hospital by way of a parenteral injection. The same needle was not sterilized and was then reused on another unsuspecting patient, thus resulting in the spread of the non-specific symptoms of disease from patient-to-patient by way of the continuous use of the same unsterlized needles. This may make some sort of sense to those who are still under the “viral” spell and are unwilling to dig a little deeper than just scratching the surface. However, for anyone looking at the evidence presented critically and logically, there is a much more reasonable explanation for the apparent outbreak of disease other than a newly discovered Ebola “virus.”
The symptoms associated with the Ebola “virus” are non-specific and mimic other diseases common to the area including influenza, malaria, yellow fever, typhoid, and even pregnancy thus the symptoms were not new or unheard of. The original patient was treated for malaria by way of an injection of chloroquine. While his malaria symptoms were said to clinically disappear after treatment, more severe symptoms showed up days later, and the patient eventually succumbed to gastrointestinal bleeding. Chloroquine is a known toxic medication with gastrointestinal problems and unusual bleeding listed as known side effects. The parenteral mode of injection is said to be risky and, if done so through the abdominal cavity, can lead to damage to the organs in the abdomen. Further patients treated at the hospital for unrelated conditions presenting with similar symptoms, including pregnant women, were also given injections of different medications, and they, too, developed the symptoms associated with severe hemorrhagic fever. Many patients were given cocktails of numerous drugs and antibiotics by way of parenteral injection. Everyone given injections at the hospital eventually died from their illnesses. The WHO even noted that those who received the injections had a different presentation of the disease than cases which were unrelated to the injections with the main difference being higher mortality in those who were treated at the hospital. It was observed that once the injections stopped, the transmission of the disease stopped as well. To anyone looking at this logically, it isn’t hard to see the connection between the injection of toxic drugs and the associated symptoms of disease. This does not require a new “virus” as an explanation yet the WHO ignored exploring parenteral injections of chloroquine and other toxic (and at least in one case experimental) drugs as a possibilty in their investigations.
When this knowledge is combined with the fact that the researchers never purified nor isolated any “virus” directly from the blood of any sick patient in Zaire as well as the fact that all of the findings from the cell cultured concoctions they created in the lab pointed to the same indirect evidence associated with the Marburg “virus” discovered less than a decade before, it is simply astonishing that they could conclude there was ever a new “virus” to begin with. The only evidence that the researchers used to claim that the Ebola “virus” was somehow a new “virus” distinct from Marburg were the Indirect Fluorescent Antibody test results which were admitted by the WHO to be less than ideal. In fact, the antibody results were all over the place with many people who never had any contact with an Ebola patient and were never sick in any way testing positive for the antibodies said to be specific to the “virus.” Meanwhile, many who had symptoms and direct contact with Ebola patients had no antibodies whatsoever. How could the results of such testing tell the researchers that they had a unique “virus?” When one understands the fraud of antibody research and that these theoretical entities have, like “viruses,” never been scientifically proven to exist, it is easy to see how the inaccurate results can be used to claim whatever the researchers want them to say. When one also realizes that the results from the antibody testing directly contradicted the Marburg findings thus showing those results to be fraudulent as well, one will understand that the CDC and the WHO were left with no choice but to try and claim a new “virus” related to Marburg was to blame in order to keep the lie about the “accuracy” of the antibody results intact.
It is pretty clear that the entire Ebola affair was one giant cover-up for the side effects brought about by toxic drugs injected parenterally. As the symptoms were non-specific and aligned with many other diseases common to the area, it was easy for the researchers to find people suffering similar symptoms in order to claim that they too were also victims of the newly “discovered” pathogenic “virus.” This pattern of covering up toxic injections with the findings of a novel “virus” was seen a decade before with the Marburg “virus” associated with Polio vaccination experimentation. They also used this same tactic to cover up poisoning by way of chemicals such as in the case with Polio and DDT/lead arsenate. Once everyone recognizes this pattern, they will be able to see right through the fraud and then we can all start working together to ensure that these tricks are no longer used to fool the gullible into fear and further poisoning by toxic drugs and injections. Together, we can break this sick cycle once and for all.

After reading about the effects of chloroquine in this article, I have a hard time taking people like Simone Gold and Robert Malone (controlled opposition, ESPECIALLY Malone) seriously when they say ANYTHING is “safe and effective(tm).” Even now, on alt-tech sites like Gab, they constantly push these poisons on us and people eat up their lies. I mean I know they are allopaths, so I throw their views out with the bath water anyway but the fact so many people still listen to them and actually BELIEVE what they say is disturbing as hell.
LikeLiked by 1 person
I believe the “safe and effective” pharmaceuticals are few and far between, if there even is such a thing. When people push these toxins as cures, I immediately suspect they are up to no good and have ulterior motives.
LikeLike
All they need are 8 willing mice and the virologists can prove anything.
LikeLiked by 1 person
Would love to see a breakdown of the supposed Anthrax pathogen in the future. With germ theory thoroughly demolished I’m now finding the case of the post-9/11 anthrax letters that were traced to Ft. Detrick incredibly enigmatic.
Another phenomenon that has me scratching my head now is infected wounds. I once was quite viciously bit on the hand by a stray cat. Dark lines appeared on my arm over the following 3-4 days, eventually reaching up to my shoulder. A doctor prescribed me antibiotics and told me I would have died if I waited longer for treatment. The lines on my arm cleared up with 48 hours after taking the pills.
As far as I’m aware cats do not possess venom so I’m now left wondering what actually happened to me. Staph infections would seem an important topic to address as well.
Both of these are (seemingly) bacteria-related, rather than “viruses”, but I’m sure I’m not the only ex-germ theory believer who would be very interested in hearing an anti-germ theory perspective on anthrax and wound infections.
LikeLiked by 1 person
Thanks for the response! I definitely plan to do more work with bacteria, hopefully starting with my next post. There is a ton of untapped potential there to explore for sure. I will see what I can uncover. 🙂
LikeLike
Thanks much.
The caption “Hiccups is a symptom of Ebola?!?!” certainly made me laugh out loud. However, they’re not listed as a symptom at the page linked to. Is there another source listing that symptom?
LikeLiked by 1 person
The image is linked to this book:
http://library.lol/main/A6AA592668A1A8E22592E4C8589C255C
From the book, it states this:
“In the context of any given Ebola outbreak, clear criteria for ETU admission should be developed, based upon the predominant manifestation of Ebola virus disease occurring at that time. These criteria need to be highly sensitive so as to keep infected individuals isolated from the rest of the community, but this will necessarily make any suspect case definition less specific and may lead to a high rate of ETU admissions among those with illnesses that mimic Ebola.
During the 2013–2015 West African Ebola epidemic, the clinical criteria for admission used in most screening algorithms consisted of:
• Fever plus at least one clinical symptom for children under 5 years of age, or
• Fever plus at least two clinical symptoms for children over 5 years of age, or
• Close contact with an Ebola suspect or case within the preceding 3 weeks.
The clinical symptoms included headache, anorexia, fatigue, musculoskeletal pain, diarrhea, nausea or vomiting, abdominal pain, difficulty swallowing, difficulty breathing, HICCUPS, and unusual or unexplained bleeding (World Health Organization 2016a).”
I also found this:
The Unlikely Clue That Led Doctors in West Africa to Ebola: Hiccups
“So many devastating, horrifying stories have come out of the ongoing Ebola crisis ravaging West Africa. This one, however, is one of the more surprising nuggets to emerge. In a new piece for Vanity Fair, journalist Jeffrey E. Stern describes the unlikely way researchers identified the disease as it first started to spread across Guinea — all thanks to a single, odd symptom: HICCUPS.”
https://www.thecut.com/2014/09/how-hiccups-helped-doctors-identify-ebola.html
So as crazy as it seems, hiccups is a symptom of Ebola. 🤣
LikeLike
Premature wound sealing is the main problem that leads to “infected wounds.” When allowed to drain properly there shouldn’t be an issue. I suspect that IF you prematurely seal, you must sterilize.
LikeLiked by 1 person
Ha ha ha ha. Reminds me of Sebastien Powell’s recent review of the Helleresque literature relating to Chicken Pox.
But this quote gets to something I’ve been curious about (yeah, I know, trying to suss the logic of virologists is akin to taking up residence in Wonderland): “My suspicion is that this would be related to the way the virus affects that body.”
Shouldn’t virologists be able to know, from looking at their EM images, what symptoms will be induced by the “infection” displayed before them? In other words, shouldn’t “CPE” look markedly different for any given virus (or at least any given virus family)?
And while we’re at it: Just as a brick cannot be seen from space but the Great Wall Of China can be, shouldn’t a viral mass, as it fills up a cell, be able to be seen in a light microscope? Like, it should be apparent, should it not, when the cell is e.g. 5%/10%/50%/80% full of viral particles? And shouldn’t the subsequent explosion be able to be witnessed as well? And shouldn’t such images be included in isolation papers?
Just some idle wondering of a Saturday night…
Thanks again for your yeoman work with this site.
LikeLiked by 1 person
You bet! Thanks for reading! 🙂
LikeLike
“We can handle Ebola safely in the hospital setting and provide the best care to the patient.”
https://www.zerohedge.com/medical/ebola-back-us-screen-passengers-uganda
LikeLike
Mike, awesome as always.
A suggestion: further up, you sometimes have one paragraph in white, then another paragraph in red, then white, then red.
It’s confusing to me which white paragraph goes with which red paragraph, whether above it or below it.
Example:
(In red)
…symptoms but had no Ebola virus antibodies. Illness in antibody-positive individuals was, in general, marked by profound
prostration, weight loss, and a convalescent period of 1-3 weeks.”
(In white)
According to the WHO, a urinary protein test, one not in use as a diagnostic today, was utilized early on in the outbreak to diagnose cases. How many of these patients were misdiagnosed based on a faulty test?
(In red)
“The only clinical laboratory test done on patients admitted to Yambuku Hospital was urinary protein. This was reported as uniformly positive and was used as a major diagnostic criterion by the nursing sisters early in the epidemic.
Maybe, you can somehow parenthesize the two that go together, which might make them easier to follow.
LikeLiked by 1 person
Thanks! I’m sorry but I’m a little confused. I don’t normally use red. Most of the time I highlight quoted sections in blue, purple, and tan. Are you reading online or on the WP Reader or somewhere else?
LikeLike
You’re right.
They are blue or tan highlights vs unhighlighted.
I checked on PC, iPhone and iPad.
Not a big thing, but thinking of the future with millions of posts historically.
LikeLiked by 1 person
The nonsenses posted by Mercola.
https://articles.mercola.com/sites/articles/archive/2023/03/28/ebola-lab-leak.aspx?ui=351b973b51dd8d94b40d43b54c99780f794c82daa03fe9c71f963a4ce91bf507&sd=20101212&cid_source=dnl&cid_medium=email&cid_content=art1HL&cid=20230328_HL2&cid=DM1366259&bid=1757073894
LikeLike