
{kind=link}
One of the oldest antivax tropes, one I recall encountering beginning soon after I started paying attention to the antivaccine movement, is that vaccines somehow cause cancer. As I wrote ten years ago, the original version of this claim derived from the observation that an early batche of the polio vaccine from the 1950s, particularly Albert Sabin’s oral vaccine, were contaminated with SV40, which led to a “cancer epidemic” over the coming decades. (SV40 is a monkey virus known as SV40, which stands for “Simian Vacuolating Virus 40” and was found to have contaminated some of the cells that the virus was grown in, specifically kidney cells derived from Asian rhesus monkeys.) The gory details aren’t important for purposes of what I’m about to discuss—and I’ve already written in depth about what happened and why this claim, although plausible because SV40 was one of the first oncogenic viruses ever discovered, turned out not to have any good evidence to support it. (Oncogenes are genes that cause cancer in experimental animals and, in some cases, humans.)
Unsurprisingly, it didn’t take long for antivaxxers to try to link COVID-19 vaccines to cancer as well, with attempts beginning even before the FDA granted an emergency use authorization (EUA) for the Pfizer vaccine two years ago. First, they falsely claimed that the mRNA vaccines “permanently alter your DNA” even though basic molecular biology should have told them that mRNA in the vaccine can’t integrate into your genome, and that the mRNA vaccines were “gene therapy, not vaccines” complete with a conspiracy theory about the CDC having supposedly changed the definition of a vaccine to include them. Next came misrepresenting old studies to claim that mRNA causes cancer. More recently, long-time antivax lawyer Thomas Renz got access to the Defense Medical Epidemiology Database (DMED), a database tracking the health of military personnel, and used it to make claims that are, at best erroneous and at worst intentionally misleading, specifically that COVID-19 vaccines have resulted in an epidemic of cancer in military personnel, including a nearly 900% increase in esophageal cancer and a nearly 500% increase in breast and thyroid cancers since before the military imposed its vaccine mandate. As I explained at the time, the claims were incredible on their face just from a scientific plausibility standpoint given that we know from the nuclear bombings at Hiroshima and Nagasaki that the cancers due to the most powerful carcinogen of all, large doses of ionizing radiation, take at least two years to begin showing up (leukemias) while most solid cancers don’t show up for around 10 years. Given that the vaccines were only introduced to the general population two years ago, even if the vaccines were as powerful a carcinogen as an ionizing radiation dose from being exposed when a nuclear bomb goes off, it would be only now that we might be beginning to see a glimmer of a cancer signal for leukemias, and even then most people didn’t receive the vaccine until months or even a year later, making too soon.
“Turbo cancer”: The new wrinkle on the vaccine-cancer lie
I suspect that even antivaxxers promoting the “COVID-19 vaccine-cancer link” probably realized—or have come to realize—deep down in what remains of their hearts the utter implausibility of their claim that COVID-19 vaccines are responsible for a wave of cancer. (At least those with any actual knowledge of cancer biology and molecular biology probably do.) That’s why, as antivaxxers often due in response to science and evidence, they have been moving the goalposts over the last few months hence the claim now that COVID-19 vaccines cause what they have dubbed “turbo cancer”. For instance:
Dr Charles Hoffe ~ “As a family doctor a small percentage of cancer patients would be diagnosed with stage 4, now 2/3rds of my cancer patients are diagnosed with stage 4
The tumours are bigger than ever they grow aggressively,spread very aggressively & are resistant to treatment” pic.twitter.com/tWw3rwf74f— Janey (@_Janey_Jay) November 14, 2022
I haven’t been able to ascertain when and by whom the term “turbo cancer” was coined with respect to COVID-19 vaccines. According to Google, use of the term dates back to at least the fall 2020, where I found it in the comments of a post about the impending EUA for the Pfizer vaccine, after which a commenter sarcastically wrote on November 30, 2020, “I can’t wait for the turbo cancer”. Unsurprisingly, besides Dr. Charles Hoffe (cited in the Tweet above), the Idaho pathologist Dr. Ryan Cole (who is also known for pushing the false COVID-19 vaccine-cancer link) uses the term, as does a Swedish pathologist named Dr. Ute Kruege. Truth be told, even though the term “turbo cancer” appears to have been bubbling around the darker depths of COVID-19 antivax conspiracy social media since sometime in 2020 at least, I didn’t start seeing it used much until early this year, and it didn’t really take off to the point of entering the mainstream zeitgeist until the summer and fall. I must admit that, as propaganda, it’s a frighteningly effective phrase, which is why I feel a bit embarrassed that I haven’t addressed the claim before.
The forms of evidence used generally consist of anecdotes and a claim that there has been a huge increase in excess mortality from cancer since the vaccines rolled out. First, let’s look at typical anecdotes, which started with pathologists like Cole and Kruege claiming that they were observing a huge increase in the number of cancers they’ve been seeing, an increase that neither has apparently seen fit to publish in the scientific literature and that other pathologists do not appear to be reporting, other than on Rumble or on antivax conspiracy sites. For instance, Kreuge claims:
Doctors for Covid Ethics posted an interview with her where she shared her concerns about unusual features that have been showing up in samples from the past year.
- Age – The average ages of the samples she received dropped, with a rise in the number of samples from people in their 30’s-50’s.
- Size – It used to be unusual for Dr. Kruger to find a tumor 3 cm in size. In this new environment, she’s regularly seeing tumors of 4 cm, 8 cm, 10 cm, and the occasional 12 cm. In a shocking anecdote, 2 weeks ago she found a 16 cm tumor that took up an entire breast.
- Multiple Tumors – Dr. Kruger has begun to see more cases of multiple tumors growing in the same patient, sometimes even in both breasts. She had 3 cases within 3 weeks of patients who had tumors growing in multiple organs. One had tumors in his/her breast, pancreas and lungs within months of getting vaccinated.
- Recurrence – There has been an uptick in patients who have been in remission from their cancer for many years, suddenly getting an aggressive recurrence of their cancer shortly after vaccination.
Of course, without actual controls, this is nothing more than the anecdotal claimed experience of two pathologists, who claim to have found a huge increase in cancer in their practices and decided that correlation (which was not shown) must equal causation because to antivaxxers it has to be the vaccines that explain any increase in a disease. It’s not good evidence of even an association between the vaccines and subsequent development or progression of cancer. In any event, let’s dig into the “turbo cancer” claim.
COVID-19 vaccines and “turbo cancer”: Hematologic malignancies
What is the difference between the more mundane antivax claims that somehow the mRNA vaccines are causing cancer and the claim that they are causing “turbo cancer”? Part of the idea is that the vaccines are somehow resulting in an epidemic of unusually aggressive fast-growing cancers (hence the term “turbo”) in young people or that they are reactivating cancers that were either in remission or previously under good control in a—you guessed it—”turbo” form that rapidly grows and spreads. For instance, check out this two minute video excerpt from one of Dr. Hoffe’s talks:
The video describes the case of a patient with an angioimmunoblastic T cell lymphoma whose cancer was reported to have started growing rapidly after he received the Moderna COVID-19 vaccine, published in November 2021 by a group of investigators in Brussels. This case report is interesting for a couple of reasons. First, it’s a great example of confusing correlation with causation. Let’s quote the case report:
A 66-year-old man with no significant medical history except for hypertension, hypercholesterolemia and type 2 diabetes presented on September 1, 2021 with cervical lymphadenopathies that became recently apparent during a flu-like syndrome. The two doses of BNT162b2 mRNA vaccine had been administered, respectively, 5 and 6 months earlier in the left deltoid. Besides moderate asthenia, he did not report any constitutional symptom. Blood examination indicated a mild inflammatory syndrome, without anemia or white blood cell changes; Lymphocytes immunophenotyping was unremarkable. Protein electrophoresis and immunoglobulin levels were normal and Coombs test was negative.
A 18F-FDG PET/CT revealed multiple voluminous hypermetabolic lymphadenopathies above and below the diaphragm as well as several extra-nodal hypermetabolic lesions (Figure 1, left panel). Considering a presumptive diagnosis of stage IV lymphoma, a left cervical lymph node biopsy was performed. Pathological examination revealed residual atrophic germinal centers, surrounded by an expanded paracortical area composed of an atypical T-cell infiltrate with clear cell morphology, expressing TFH cell markers (CD3, CD4, PD1, ICOS, BCL6, CXCL13) and a loss of CD7. The paracortical area contained an increased number of high-endothelial venules, supported by an increased number of follicular dendritic cell networks, with some foci of EBV+ B-cell immunoblastic proliferation in the background (Figure 2). These features highly suggested a diagnosis of AngioImmunoblastic T cell Lymphoma (AITL), pattern 2.
So this man was diagnosed with an angioimmunoblastic T cell lymphoma six months after having received the Moderna vaccine. This particular form of lymphoma is described as a “rare, often but not always, aggressive (fast-growing) form of peripheral T-cell lymphoma (PTCL).” It’s also a disease that is almost always advanced when it is first diagnosed, either stage III or IV. Its prognosis is generally poor, with “disease relapse and infections” being “common with this cancer,” and a five year overall survival (OS) of 63% and progression-free survival (PFS) of 41% for low risk disease, which fall to an OS of 21% and 13% for high risk disease. So right off the bat, this patient had a poor prognosis at the time of diagnosis.
Here’s what happened next:
Fourteen days after the PET/CT, a booster dose of the BNT162b2 mRNA vaccine was administered in the right deltoid in preparation of the first cycle of chemotherapy. Within a few days following the vaccine booster, the patient reported noticeable swelling of right cervical lymph nodes. In order to get a baseline close to the initiation of the therapy, a second 18F-FDG PET/CT was performed 8 days after the vaccine booster administration, i.e. 22 days after the first one.
Here’s the image:
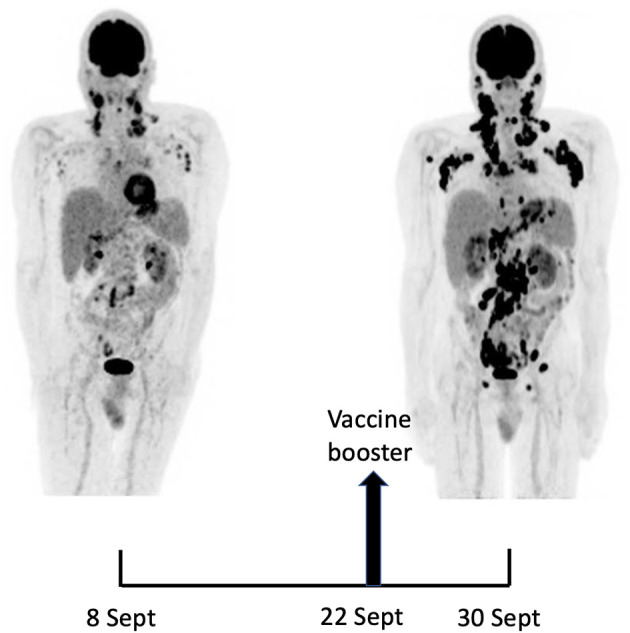
Figure 1. Maximum-intensity-projection images of 18F-FDG PET/CT at baseline (8 Sept) and 22 days later (30 Sept), 8 days after BNT162b2 mRNA vaccine injection in right deltoid. 8 Sept: hypermetabolic lymph nodes mainly in the supra-clavicular, cervical, and left axillary regions; restricted gastro-intestinal hypermetabolic lesions. 30 Sept: Dramatic increase in nodal and gastro-intestinal hypermetabolic lesions. Asymmetrical metabolic progression in the cervical, supra-clavicular and axillary area, more pronounced on the right side.
For those who haven’t seen PET scans before, the black areas are areas that take up the tracer and are therefore more metabolically active. Given that cancer cells are generally more metabolically active than normal cells, this indicates an increase in the extent of the cancer (other than the brain, which is highly metabolically active normally). Of course, just as likely, if not more so, is the possibility that the tumor was rapidly growing at the time of diagnosis and the vaccine had nothing to do with its rapid progression over 22 days. Indeed, it strains credulity that anything could cause such rapid progression in a mere eight days.
The authors speculated that the mRNA from the vaccine had gotten to the lymph nodes under the arm (axillary lymph nodes) and somehow fired up the cancer. By way of background, it is known that injection of COVID-19 vaccines in the shoulder can, because of the lymphatic drainage patterns of the arm, lead to lymphadeopathy (enlargement of the lymph nodes) under the arm, due to inflammation and immune reaction to the vaccine, a phenomenon that was soon found to interfere with the interpretation of routine screening mammograms. The authors noted that, on biopsy, the “pathological picture showed reactive benign changes with prominent germinal centers.” The authors speculated that somehow the vaccine stimulated T follicular helper (TFH) cells and somehow promoted cancer growth:
In fact, the supposed enhancing action of the vaccine on AITL neoplastic cells is fully consistent with previous observations identifying TFH cells within germinal centers as key targets of nucleoside-modified mRNA vaccines both in animals and in man (1, 2). Malignant TFH cells, the hallmark of AITH, might be especially sensitive to mRNA vaccines when they harbor the RHOA G17V mutation which was present in our case. Indeed, this mutation facilitates proliferation and activation of several signaling pathways in TFH cells (16). Furthermore, mice genetically engineered to reproduce the RHOA G17V and TET2 mutations—both were present in our case—develop lymphoma upon immunization with sheep red blood cells (16). This experimental observation is relevant to RNA vaccines as RNA of sheep red blood cells was shown to be responsible for their ability to stimulate TFH and induce germinal center reaction (17).
Antivaxxers generally do not mention that the authors also wrote that “extrapolation of the findings of this case to other patients with AITL or other peripheral T cell lymphoma involving TFH cells is premature” because “AITL patients are rare and their mutation profile is heterogeneous” and “their immune reactions might be affected by their treatment,” while concluding that, whatever the result of further studies of the effect of mRNA vaccines on AITL, “it should not affect the overall favorable benefit-risk ratio of these much-needed vaccines.” In any event, this case report did involve a lot of handwaving and speculation, which led me to ask: Have followup studies (unmentioned, of course, by antivaxxers) supported this idea?
The answer is: Not much. There’s a case report of recurrence of a primary cutaneous CD30-positive lymphoproliferative disorder following COVID-19 vaccination that doesn’t show evidence of causation. There’s also a case report of two hematologic malignancies diagnosed in the context of the mRNA vaccination campaign published in June, a case of a diffuse large B-cell non-Hodgkin lymphoma diagnosed one week after her second dose dose of the Pfizer vaccine and a case of T/NK lymphoma manifested on the third day after the initial dose of the Pfizer vaccine. The rapid sequence implies, more than anything else, that these diagnoses were likely coincidence, with the authors themselves pointing out, “The link between the two events reported is only temporal,” adding that “any clinical event, especially when associated with novel vaccines or treatments, should be reported, as this is the starting point for additional investigations of particular mechanisms of action, thus consolidating knowledge about the safety profile, to the benefit of the patients.” Overall, there is no evidence suggesting causation of hematologic malignancies by COVID-19 vaccines, and the changes in lymph nodes observed are generally benign.
There’s another anecdote, published by Roxanne Khamsi in The Atlantic (which, unfortunately, has “balanced” great pandemic reporting by Ed Yong and others with outright conspiratorial nonsense) titled “Did a famous doctor’s COVID shot make his cancer worse?” The article featured one of the patients from the case report of the angiolymphatic T-cell lymphoma report, who turned out to be Michel Goldman, described as a “Belgian immunologist and one of Europe’s best-known champions of medical research.” One thing I learned reading the article is that Goldman is rather naïve:
“I would say that 95 percent of the reactions were extremely friendly,” Michel told me later. But as he’d feared, anti-vaccine activists picked up on the story. “The lymph nodes of those who have taken these shots are exploding, burgeoning, and bulging with this toxic bioweapon,” a right-wing influencer named Jane Ruby wrote on Telegram beneath a screenshot of Michel’s CT scans, which had appeared in his published paper (and are reproduced in this article). “LYMPHOMA – That’s right… Cancer of the lymphatic system … STOP THIS FROM GETTING INTO BABIES AND CHILDREN!!!!!” Ruby’s claims were amplified on Natural News, among other anti-vaccination sites where, again, the very images that Michel’s brother had used to diagnose his illness were presented as shocking evidence of vaccination’s dangers. “PHOTOS: LYMPHOMA CANCER EXPLODING IN THE BOOSTED,” one website said.
When I told Michel about these online posts, he shook his head in disappointment. “They’re looking for anything to support their crazy vision,” he said. “It makes me sad about the world in which we are living.” That’s not to say he was surprised. Michel knew, for instance, that medical experts have dispelled false rumors about vaccines infecting people with COVID-19. He told me that he’d obsessed over getting the tone of the manuscript exactly right, so as not to fuel vaccine skepticism. He was careful, for example, to describe the vaccine as possibly “inducing” the “progression” of his cancer—rather than “causing” it to surface. “I spent hours and hours,” he said. “I’ve never spent so much time on details in a paper.”
I could have told Goldman that it wouldn’t have mattered how he and his brother phrased the case report, that it would have been used the way it was used regardless. I’ll also say that, having read the case report, I can’t honestly say that the article wasn’t written clearly enough to make it sound as though Goldman and his brother were speculating that the vaccine might have “induced” the “progression” of his tumor. Moreover, whether or not they realized it, Goldman and his brother actually handed antivaxxers another talking point to replace the antivax claim that the COVID-19 vaccines were causing cancer with a more credible-seeming claim that they were fueling “progression” of “turbo cancer” in people who already had it, particularly those whose cancers were either in remission or had been growing slowly or not at all under treatment. None of this is to say that his case report shouldn’t have been published, just that Goldman shouldn’t have been the least bit surprised by how his case report was weaponized by the antivaccine movement, particularly given this speculation that was in the paper but that I quote from the Atlantic article because it’s more layperson-friendly:
He also came across another, very important clue. In 2018, a team of researchers based at Columbia University’s Institute for Cancer Genetics had published an intriguing study using mice with a pair of gene mutations that, when they co-occur, predispose T cells to go rogue. (Michel’s tumor, which had been sequenced by this point, showed the same two mutations.) When these mice were injected with sheep red-blood cells—as an experimental stand-in for invading microbes—the animals developed the subtype of lymphoma that was diagnosed in Michel.
Now Michel had a theory to explain the bleak coincidence that had befallen him. Serge agreed that it made sense. The brothers had co-written research papers in the past, including ones on the use of stem cells for heart repair and dendritic-cell vaccines for cancer. It was time for them to write another.
Again, speculation of a link and what mechanism might account for it is not inappropriate in the scientific literature, but no one should be surprised when that link and the mechanism become antivax talking points. Goldman can go on Belgian TV all he likes and say that vaccination is safer than not being vaccinated, but he should realize that his contributing to an article like this one in The Atlantic actually undermines his message, given the bothsidesism in the reporting. While the report did correctly point out how difficult it is to report on potentially rare side effects of a vaccine, in my assessment it gave a bit too much attention to Goldman’s speculative claim, although I was very happy to see that Goldman was doing well when the article was written.
Other “theories” of causation
I will note that Goldman’s idea is not the only speculative “theory” that antivaxxers tout. For example, Ryan Cole—the Idaho pathologist whom we’ve met before spreading the claim that he’s seeing lots and lots more cancer, which he attributes to COVID-19 vaccines, of course:
According to Cole, human cells have so-called toll-like receptors (TLRs) that classify whether a foreign object in the body is harmful or not. “When the [COVID-19] shots go into the body, they turn some of these [TLRs] off. Normally, they have to be on,” he said.
The pathologist added that when the vaccines turn off some of these TLRs, the immune system’s alert mechanism is compromised as a result. TLR7 and TLR8 are in charge of detecting viruses, while TLR3 and TLR4 are responsible for keeping cancer in check.
I’ve discussed before that this is a misrepresentation of the science in that the modified RNA used in the mRNA vaccines do not change the ability of the immune system to recognize anything other than the modified mRNA:
The UK Column article claimed that the study used RNA modifications to “turn off [T]oll-like receptors”. But no such thing is described in the study by Karikó et al. The modifications and their effects are associated with the modified RNA only, and don’t change the ability of TLRs to detect other microbial components.
To use an analogy, modifying RNA is like putting on camouflage to evade detection by sentries guarding a border. But those sentries remain capable of detecting other intruders that don’t have the camouflage.
Furthermore, as Karikó et al. noted, the modifications used in the study are also observed in nature, and mammalian RNA is naturally replete with such modifications. If the article’s claim that such modifications weaken the immune system were true to begin with, then such pre-existing modifications alone would be enough to weaken the immune system even without the COVID-19 vaccines.
In short, the article misrepresented the study’s findings and is inconsistent with real-world observations.
Cole, I note, basically parrots the claim in the article cited in the excerpt above, and adds to it this claim:
Furthermore, he pointed out that the SARS-CoV-2 spike protein binds to the P53 gene – the so-called “guardian of the genome” – which suppresses tumors. The spike protein’s S1 subunit also binds to the TMPRSS-2 gene linked to prostate cancer in men and the BRCA genes linked to breast cancer in women.
“We’re giving a shot that makes a spike protein. That’s a toxin that triggers cancer genes in bad ways and turns off other pattern receptors,” Cole told the New American contributor. “We don’t know how long the immune system is suppressed after these shots and how long these receptors are shut off – because those studies aren’t done.”
p53 is indeed arguably the most important tumor suppressor gene. Genetic syndromes in which p53 function is decreased or eliminated do, in fact, lead to a vastly increased risk of a number of cancers. Where did Cole get this claim from? There is evidence that SARS-CoV-2 infection can lead to downregulation (decreased production/activity) of p53, suggesting that persistent COVID-19 infection could be a risk factor for developing cancer because of lower P53 levels detected in patients with severe COVID-19 and long COVID. There is also an in silico (computer modeling) study from 2020 suggesting that the spike protein can interact with p53.
A recent review article notes:
A direct interplay between p53 and SARS-CoV-2 has been suggested for the first time following an in silico study reporting on the ability of the S2 subunit of the virus to physically and strongly interact with p53 (Singh and Bharara Singh, 2020). In the same line, another mechanism of interaction has been highlighted in a large animal model study showing that p53 can regulate ACE2 receptor in a tissue- and sex-specific fashion (Zhang et al., 2021). It is of interest that the reported higher expression of ACE2 in females can be related to estrogens activity, and perhaps contributing to the lower disease susceptibility of females compared to males (Bonaccorsi et al., 2020). Thus, this first level of interactions between p53 and SARS-CoV-2 occurs via the modulation of ACE2 expression in a sex-related manner and via a direct interaction between the S2 subunit of the viral spike protein and p53, although the significance of this interaction has not been addressed so far. Of note, a direct regulatory activity of p53 on SARS-CoV-2 replication is a shared feature characterizing other previous coronaviruses (Ma-Lauer et al., 2016).
Note that, first, all of this, even if it pans out, says nothing about the vaccine; rather, it is about persistent SARS-CoV-2 infection, not vaccination. The vaccine only transiently produces the spike protein, which is rapidly externalized. If it weren’t externalized, then it wouldn’t be able to provoke an immune response. p53 is not just an intracellular protein, but, unlike the spike protein, is primarily an protein of the nucleus. Vaccination is transient by nature, and, even if this proposed interaction were relevant, would require prolonged interaction between spike and p53. Basically, this is antivaxxers doing what antivaxxers like to do, pulling a claim out of their nether regions and then looking for scientific studies that can be twisted to support that claim, no matter how tenuous the support, leading to headlines like this one from Mike Adams, “THE VACCINE-CANCER ATROCITY: Like clockwork, most vaccinated Americans will lose immune function by Christmas and start growing accelerated CANCER tumors that will kill them over the next ten years“.
Let’s just say that I’ll take my chances.
Excess mortality
Another claim going around to support the conspiracy theory that the vaccines are causing “turbo cancer” comes from—among other sources—the horribly self-named The Ethical Skeptic (TES). The claims coming from TES arise from his incompetent analysis of CDC provisional death statistics. I might have to go into the claims in more detail in a subsequent post, but for now let me just thank Prof. Jeffrey Morris for deconstructing these claims almost four months ago so that I don’t have to do so now, given how long this post has become.
Prof. Morris notes first:
An anonymous, apparently very experienced and prolific analytical systems modeler who is heavily followed on twitter, @EthicalSkeptic, has been modeling the publicly CDC provisional deaths by cause data for the past 6 months, and concludes from his models that a specific factor (which must not be named) in early Spring 2021 introduced an inherent change point into the data leading to increasingly high numbers of excess deaths in the USA…These posts have been very influential, with many touting them as evidence of serious harm, and others dismissing them outright. The lack of detailed documentation of the analytical steps make it difficult for others to evaluate his model and conclusions.
Unfortunately, although TES blocked me on Twitter making it hard for me to verify, this does appear to be true. In any event, Prof. Morris carefully looks at TES’s claims and finds them…lacking. First, it’s very instructive to look at one of Prof. Morris’s many graphs:
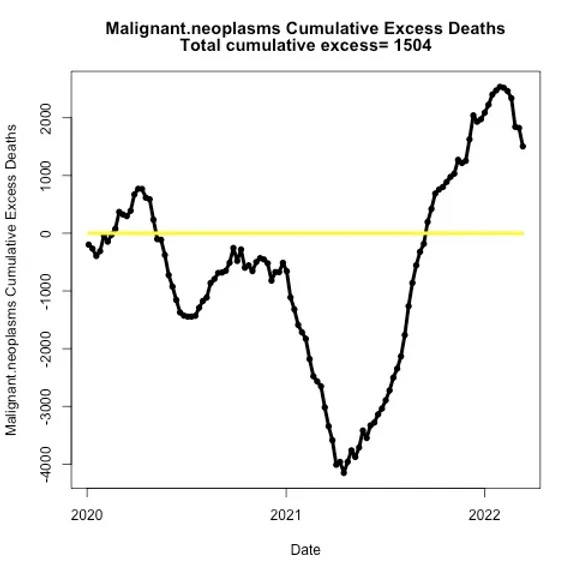
Professor Morris’ estimate of excess cancer deaths using the TES dataset,
Prof. Morris observes:
We see how the the mid-2020 and early 2021 major deficits resulted in ~4k deficit cancer deaths relative to baseline since the beginning of the pandemic by spring 2021, which recovers all the way to baseline by late 2021 and reaches a maximum of ~2k excess cancer deaths by early 2022, after which it starts to decline again.
Based on these data and the proposed seasonal/annual linear baseline, there were major deficits of cumulative cancer deaths during the pandemic relative to baseline through Spring 2021, which then recovered and moved into excess territory in early 2022, with about 2k excess (which is <2 days of cancer deaths at the baseline 11.5k weekly rate).
In other words, a lot of this could be reporting artifacts, specifically delays in reporting and changes in screening due to the pandemic could explain a lot of this:
Many oncologists have stated that the delaying of cancer screenings/preventative care during the pandemic could lead to an eventual increase in cancer deaths, with cancers diagnosed later, but at a later and less treatable stage. Indeed this may occur and may be starting to occur, but is not fully apparent yet in these data.
Of course, those claiming high excess cancer deaths including @EthicalSkeptic are not considering that factor, but are claiming it is due to another “must not be named factor” starting in Spring 2021. Based on my understanding of carcinogenesis from >25 years of experience in cancer research, even after a major carcinogenic insult, I would not expect it to lead to a high number of excess cancer deaths for many years given the time it typically takes to for cancer to initiate, develop, become advanced, and lead to death even in cases of extreme established carcinogens.
In order to advance such a claim for this unnamed factor, one would need to at least have a plausible hypothesis and some evidence for how this factor could produce advanced cancers and deaths so quickly, beyond near-baseless speculation.
Prof. Morris is echoing a point that I’ve made many times. Even in the highly unlikely event that COVID-19 vaccines (or even, as I discussed above, COVID-19 itself) can somehow predispose people to cancer, this increase in cancer incidence would not be expected to manifest itself for several years. Even if the “analysis” (if you can call it that) by TES is epidemiologically appropriate (which is doubtful), it is far more likely that something else accounts for the increase in excess mortality besides COVID-19 vaccines, as much as antivaxxers do what they want to do and find a way to blame vaccines for something bad, particularly in the middle of a pandemic that has already caused so many bad things to happen and is continuing to do so.
There is no such thing as “turbo cancer”
Unsurprisingly, “turbo cancer” isn’t a thing. Oncologists don’t recognize it as a phenomenon, nor do cancer biologists, and if you search for it on PubMed, you won’t find a reference to it. Basically, it’s a clever term coined by antivaxxers to scare you into thinking that COVID-19 vaccines will give you cancer, or at least greatly increase your risk of developing cancer. The “evidence” marshaled to support the concept consists of the usual misinformation techniques used by antivaxxers: citing anecdotes, wild speculation about biological mechanisms without a firm basis in biology, and conflating correlation with causation, no matter how much one must squint to see it.
Unfortunately, “turbo cancer” is also too frightening and pithy of a term to go away any time soon. I expect antivaxxers to be using it for years to come, perhaps for the rest of my life.