




Discover more from Protons 101
OAR metrics demonstrating correlation to clinical outcomes (REFERENCE SERIES)
Proposed reference document PRODOSC trial concept - 65+ references included.

Work of one: massive project scope. Please comment any suggestions or improvements. Long-term goal is living reference document.
Today’s article is a reference piece of material that attempts to compile previously demonstrated important dosimetry metrics that POTENTIALLY could reveal and advantage for avoidance with proton therapy. Essentially we begin with CNS and work inferiorly.
This work was done as part of the development of the PRODOSC trial concept in which patients would be analyzed or randomized based on improving previously “validated” dosimetry metrics based on radiation oncology literature.
I’ve included a brief overview of the proposed trial structure. Please see the full post linked below for further details and documentation.

ELIGIBILITY:
Age: 65 or older
Concurrent Chemotherapy during radiation
Traditional fractionation to definitive dosing (<2.2 Gy or RBE(Gy))
Definitive goal. (Can be pre / post-operative. Can have oligometastatic disease so long as the intent is to treat all disease in a definitive fashion.)
Anticipated Main Sites:
CNS, Head and Neck, Esophagus, Lung, Pancreas, Hepatobilliary, Colo-Rectal, Cervix, Bladder, Anal (Note: These sites then becomes the OAR metric sections below)
Primary Outcome: Reduced Toxicity (Acute and 3 yr)
Acute CTCAE: 90 - Day Grade 3 or higher toxicity
3 year - CTCAE Gr3 or higher toxicity
Secondary Outcomes:
PFS
OS - 3 yr and 90 day mortality
90-day Grade 4 Lymphopenia
Long Term Toxicity 3yr
ECOG score
Charlson-Deyo Comorbidity score
Eq-5D-3L Patient Reported Outcomes
Per the proposed structure, OAR metrics should fulfill three goals: 1) they should be reasonably balanced across the included disease site, 2) they should demonstrate data linking the proposed metric to clinical outcomes. 2) proton therapy should have dosimetric data demonstrating an ability to differentiate plans from IMRT plans based on the metric.
Initial Proposed Dosimetry Metrics Including “Best” Supporting Literature References:
CNS brain constraint >100cc diff in 10Gy
Hippocampus Highest Mean <10 Gy
Posterior fossa <10Gy mean
Pituitary <30 Gy
Cochlea Highest Mean dose <25 Gy
Oral cavity Mean dose reduction 50%
Parotid Highest mean <20 Gy
Pharyngeal Constrictors (SMPCM and IPCM) mean<50 Gy and <20 Gy respectively
Esophagus Mean dose 20% reduction
Lung v5<55% (requiring a v20<20%)
Mean Heart Dose<10Gy
LAD v15 <10%
Liver 30% reduction mean dose
Bowel(within 5 cm of GTV) 30% reduction mean dose
Rectum v50 20% reduction
Bone Marrow v20 50% reduction
Immune System 1 nomogram risk group reduction
Notations:
* Means bilateral structure. The intent is that each side of the bilateral structure must meet the constraint.
“Best” is quoted due to scope of project. Likely hundreds of references can / could add value and certainly the OAR and the OAR metrics are debatable as well. Min of 3 per OAR included.
CNS brain constraint >100cc difference in volume treated to 10Gy; (brain minus PTV)
Example: IMRT plan delivers 10 Gy to 250cc of normal brain and Proton plan delivers 10Gy to 149cc.
Supporting Data Strength (1 weakest: 5 strongest): 1
Comment: Very little data supporting normal brain as a constraint. The two strongest references are the hippocampal sparing data vs WBRT and the pediatric medulloblastoma data both of which really lack a CNS metric. One would think there are important metrics in the brain, but they are poorly defined currently. The one chosen is best described as an informed guesstimate.
References:
Superior Intellectual Outcomes After Proton Radiotherapy Compared With Photon Radiotherapy for Pediatric Medulloblastoma
DOI: 10.1200/JCO.19.01706Dosimetric Comparison of Intensity-Modulated Radiotherapy versus Three-Dimensional Conformal Radiotherapy for Patients with Brain Tumors
DOI: 10.4236/ojrad.2014.41011Efficacy of Stereotactic Conformal Radiotherapy vs Conventional Radiotherapy on Benign and Low-Grade Brain Tumors A Randomized Clinical Trial
DOI: 10.1001/jamaoncol.2017.0997A comparative study of dose distribution of PBT, 3D-CRT and IMRT for pediatric brain tumors
DOI: https://doi.org/10.1186/s13014-017-0775-2A dosimetric comparison between three-dimensional conformal radiation therapy and intensity-modulated radiation therapy in the treatment of posterior fossa boost in medulloblastoma.
DOI: 10.4103/0973-1482.220416.
Hippocampus* Mean dose <10 Gy
Example: Contralateral Hippocampus- both plans meet dose level <10 Gy. Ipsilateral IMRT plan delivers a mean dose of 11 Gy and the Proton plan delivers an ipsilateral mean dose of 7 Gy.
Supporting Data Strength (1 weakest: 5 strongest): 4
Comment: There is clearly emerging data that protection of the hippocampus delivers improved outcomes. The NRG CC001 is clear randomized prospective data making it arguably the strongest single avoidance data. It is downgraded here as that approach is markedly different than an IMRT vs. Proton for definitive treatment in a partial brain setting.
References:
Hippocampal Avoidance During Whole-Brain Radiotherapy Plus Memantine for Patients With Brain Metastases: Phase III Trial NRG Oncology CC001.
DOI: https://doi.org/10.1200/JCO.19.02767Whole Brain Radiotherapy With Hippocampal Avoidance and Simultaneously Integrated Brain Metastases Boost: A Planning Study
DOI: https://doi.org/10.1016/j.ijrobp.2007.05.038Hippocampal-Sparing Whole-Brain Radiotherapy: A “How-To” Technique Using Helical Tomotherapy and Linear Accelerator–Based Intensity-Modulated Radiotherapy DOI: https://doi.org/10.1016/j.ijrobp.2010.01.039
Posterior fossa <10Gy mean
Example: IMRT plan dose of 11 Gy and Proton plan delivers mean dose of 2 Gy.
Supporting Data Strength (1 weakest: 5 strongest): 3
Comment: Literature review often coming from the development phase of IMRT in head and neck cancer points to increased nausea with the move from 3D to IMRT. This is thought to be related to increased dose to the posterior fossa with IMRT plans and is a consistent finding in the early 2000’s literature from major institutions. Proton therapy seems to reduce that nausea and delivers less dose to the brainstem and posterior fossa but exact data for this metric is far from defined.
References:
Proton Radiation Therapy for Head and Neck Cancer: A Review of the Clinical Experience to Date DOI: https://doi.org/10.1016/j.ijrobp.2014.02.029
Proton radiation for treatment of cancer of the oropharynx: Early experience at Loma Linda University Medical Center using a concomitant boost technique DOI: https://doi.org/10.1016/j.ijrobp.2004.09.064
Dosimetric Comparison of IMRT and Proton Therapy for Head and Neck Tumors DOI:10.1016/j.ijrobp.2006.07.772
Pituitary mean dose <30 Gy
Example: IMRT plan dose of 32 Gy and Proton plan delivers mean dose of 26 Gy.
Supporting Data Strength (1 weakest: 5 strongest): 2
Comment: Good data supporting loss of function with higher doses. Most data stems from younger populations and not the trial target population therefore weakening strength. Data supports dose ranges from 30 Gy to 50 Gy. We purposefully choose at the lower end of this spectrum as planning has likely improved from these papers. Very questionable that it will relate to measurable Gr2/Gr3 toxicity in this population.
References:
Hypothalamic/pituitary function following high-dose conformal radiotherapy to the base of skull: demonstration of a dose–effect relationship using dose–volume histogram analysis DOI: https://doi.org/10.1016/S0360-3016(00)01387-0
Endocrine Outcomes for Children With Embryonal Brain Tumors After Risk-Adapted Craniospinal and Conformal Primary-Site Irradiation and High-Dose Chemotherapy With Stem-Cell Rescue on the SJMB-96 Trial
DOI: 10.1200/JCO.2008.13.5293Fertility of Female Survivors of Childhood Cancer: A Report From the Childhood Cancer Survivor Study DOI: 10.1200/JCO.2008.20.1541
Cochlea* Highest Mean dose <30 Gy
Example: Contralateral Cochlea - both plans meet. Ipsilateral IMRT plan delivers a mean dose of 33 Gy and the Proton plan delivers an ipsilateral mean dose of 27 Gy.
Supporting Data Strength (1 weakest: 5 strongest): 2
Comment: Stronger dosimetry metrics than many sites, but rather wide dose levels to as high as 45-50 Gy. Combined with the lack of certainty that toxicity will be a measurable effect at 3 years of follow-up, it is a low rated metric despite better than average dosimetry publication data. Population in trial makes less critical as much is measured but subclinical effects.
References:
Organs at risk in the brain and their dose-constraints in adults and in children: A radiation oncologist’s guide for delineation in everyday practice. https://doi.org/10.1016/j.radonc.2015.01.016
Normal tissue complication probability modeling for cochlea constraints to avoid causing tinnitus after head-and-neck intensity-modulated radiation therapy. https://doi.org/10.1186/s13014-015-0501-x
Cochlea sparing effects of intensity modulated radiation therapy in head and neck cancers patients: a long-term follow-up study
https://doi.org/10.1186/s40463-014-0030-xTolerance of Normal Tissue to Therapeutic Radiation.
https://applications.emro.who.int/imemrf/Rep_Radiother_Oncol/Rep_Radiother_Oncol_2013_1_1_35_48.pdf
Oral cavity: 25% reductions in mean dose.
Example: IMRT plan delivers mean dose of 25 Gy and Proton plan delivers mean dose of 18.75 Gy or less.
Supporting Data Strength (1 weakest: 5 strongest): 3
Comment: There is less data on this structure than anticipated. Dose clearly causes treatment related toxicity. The structure is rather inconsistently contoured and metrics are poorly defined but the recent UNC publication adds strength. It is an area where protons and IMRT plans differ significantly from a dosimetry standpoint and therefore included.
References:
Acute toxicity in comprehensive head and neck radiation for nasopharynx and paranasal sinus cancers: cohort comparison of 3D conformal proton therapy and intensity modulated radiation therapy
DOI: https://doi.org/10.1186/s13014-016-0600-3Quality of Life of Postoperative Photon versus Proton Radiation Therapy for Oropharynx Cancer DOI: 10.14338/IJPT-18-00032.1
Impact of Oral Cavity Dosimetry on Patient Reported Xerostomia and Dysgeusia in the Setting of Deintensified Chemoradiotherapy DOI: 10.1016/j.adro.2022.100952
Parotid* Highest mean or cumulative mean <15 Gy
Example: Contralateral Parotid - both plans meet. Ipsilateral IMRT plan delivers a mean dose of 18 Gy and the Proton plan delivers an ipsilateral mean dose of 14 Gy. Or IMRT delivers combined parotid mean dose of 21Gy and the proton plan delivers dose of 14Gy.
Supporting Data Strength (1 weakest: 5 strongest): 4
Comment: Rated at strong due to the fact that this single metric was utilized to defend IMRT treatment. Somewhat surprisingly, there is early data and then nearly a decade gap to some of the newer attempts to better define metics for current planning.
References:
Prospective Randomized Study of Intensity-Modulated Radiotherapy on Salivary Gland Function in Early-Stage Nasopharyngeal Carcinoma Patients
DOI: 10.1200/JCO.2007.11.5501Target Volume Definition for Head and Neck Intensity Modulated Radiotherapy: Pre-clinical Evaluation of PARSPORT Trial Guidelines
DOI: https://doi.org/10.1016/j.clon.2007.07.001Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer (PARSPORT): a phase 3 multicentre randomised controlled trial DOI: https://doi.org/10.1016/S1470-2045(10)70290-4
Dose/Volume histogram patterns in Salivary Gland subvolumes influence xerostomia injury and recovery DOI: https://doi.org/10.1038/s41598-019-40228-y
A Model-Based Method for Assessment of Salivary Gland and Planning Target Volume Dosimetry in Volumetric-Modulated Arc Therapy Planning on Head-and-Neck Cancer DOI: 10.4103/jmp.JMP_19_19
A Nomogram to predict parotid gland overdose in head and neck IMRT
DOI: https://doi.org/10.1186/s13014-016-0650-6Dose-volume modeling of salivary function in patients with head and neck cancer receiving radiotherapy. Int J Radiat Oncol Biol Phys 2005;62:1055–1069
https://pubmed.ncbi.nlm.nih.gov/15990009/
Pharyngeal Constrictors: Superior Middle Pharyngeal Constrictor Muscle mean < 50 Gy; Inferior Pharyngeal Constrictor Muscle mean <20 Gy
Example: IMRT delivers mean dose to SMPCM 52 Gy and Proton plan delivers 46 Gy. Or for the IPCM, IMRT mean dose 22 Gy and Proton plan with 18 Gy.
Supporting Data Strength (1 weakest: 5 strongest): 5
Comment: The DARS trial has been presented in abstract form demonstrating the above metrics result in clinical outcome improvements in MDADI. The data illustrating that protons can further reduce dosing is my own work published here on this Substack. References include work demonstrating this metric is difficult to meet with IMRT.
References:
Nutting C, Rooney K, Foran B, et al on behalf of the DARS Investigators. Results of a randomized phase III study of dysphagia-optimized intensity modulated radiotherapy (Do-IMRT) versus standard IMRT (S-IMRT) in head and neck cancer. J Clin Oncol May 20, 2020; 38(15_suppl) 6508-6508.
DOI: 10.1200/JCO.2020.38.15_suppl.6508Petkar I, Rooney K, Roe JWG, et al. DARS: a phase III randomised multicentre study of dysphagia- optimised intensity- modulated radiotherapy (Do-IMRT) versus standard intensity- modulated radiotherapy (S-IMRT) in head and neck cancer. BMC Cancer. 2016;16:770. https://doi.org/10.1186/s12885-016-2813-0
Can Dysphagia Aspiration Related Structures (DARS) Be Spared In Patients With Oropharyngeal Cancers? Dosimetric Evaluation In A Prospective Study Of DARS Optimized Intensity Modulated Radiation Therapy
https://www.researchsquare.com/article/rs-1864509/v1.pdfStorey MR, Rana S. Dysphagia-Optimized Unilateral Proton Radiation Therapy: A Comparative Study Evaluating Constrictor Muscle Dosimetry URL.
Esophagus Mean dose 20% reduction
Example: IMRT plan delivers mean dose of 20 Gy and Proton plan delivers mean dose of 16 Gy or less.
Supporting Data Strength (1 weakest: 5 strongest): 4
Comment: One of the few proven metrics via a prospective trial demonstrating direct impact on clinical outcomes. The prospective trial was in palliative cases but reducing dose to 80% of prescription resulted in less esophagitis with more impact with higher dose. Other references are less consistent and therefore, strength moved to 4 for our definitive dose trial structure.
References:
Palliative Radiation for Advanced Central Lung Tumors With Intentional Avoidance of the Esophagus (PROACTIVE)A Phase 3 Randomized Clinical Trial
https://jamanetwork.com/journals/jamaoncology/fullarticle/2789387Multi-Institutional Prospective Study of Reirradiation with Proton Beam Radiotherapy for Locoregionally Recurrent Non–Small Cell Lung Cancer
DOI: https://doi.org/10.1016/j.jtho.2016.10.018Treatment-related Acute Esophagitis For Patients With Locoregionally Advanced Non–Small Cell Lung Cancer Treated With Involved-field Radiotherapy and Concurrent Chemotherapy DOI: 10.1097/COC.0b013e31827de7a2
Long-Term Results of NRG Oncology RTOG 0617: Standard- Versus High-Dose Chemoradiotherapy With or Without Cetuximab for Unresectable Stage III Non–Small-Cell Lung Cancer DOI: 10.1200/JCO.19.01162
Lung v5<55% (requiring a v20<20%)
Example: IMRT plan delivers lung dosimetry of v20 of 18% and v5 of 75%. Proton plan delivers v20 of 19.5% and v5 of 52%.
Supporting Data Strength (1 weakest: 5 strongest): 3
Comment: In light of the Bayesian Adaptive study, the most interesting paper is the first which combines moderate and low dose metrics into a predictive model. What once was an early strong and consistent dosimetry metric that potentially could be a strong opportunity for proton therapy to reduce toxicity, it appears much less likely that reduction in lung volumes will be a primary driver of use but lung dose likely helps drive more broad reaching toxicity metrics.
References:
Combined Analysis of V20, VS5, Pulmonary Fibrosis Score on Baseline Computed Tomography, and Patient Age Improves Prediction of Severe Radiation Pneumonitis After Concurrent Chemoradiotherapy for Locally Advanced Non–Small-Cell Lung Cancer DOI: https://doi.org/10.1097/JTO.0000000000000187
Bayesian Adaptive Randomization Trial of Passive Scattering Proton Therapy and Intensity-Modulated Photon Radiotherapy for Locally Advanced Non–Small-Cell Lung Cancer DOI: 10.1200/JCO.2017.74.0720
Impact of Intensity-Modulated Radiation Therapy Technique for Locally Advanced Non–Small-Cell Lung Cancer: A Secondary Analysis of the NRG Oncology RTOG 0617 Randomized Clinical Trial DOI: 10.1200/JCO.2016.69.1378
Mean Heart Dose Improvement of 2 Gy
Example: IMRT plan delivers mean heart dose of 12Gy and the proton plan delivers a dose of 9Gy.
Supporting Data Strength (1 weakest: 5 strongest): 5
Comment: Arguably the current gold standard for a dosimetry relating directly to outcome despite having no randomized controlled studies. The RADCOMP trial will probably be the best data source in the near future. Strength is based on consistency of retrospective data. Cardiac subtructure dosimetry data continues to build, yet, mean heart dose often continues to hold up as a outcome predictor.
References:
Cardiac Radiation Dose, Cardiac Disease, and Mortality in Patients With Lung Cancer https://doi.org/10.1016/j.jacc.2019.03.500
Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): a randomised, two-by-two factorial phase 3 study. DOI: 10.1016/S1470-2045(14)71207-0
Impact of Intensity-Modulated Radiation Therapy Technique for Locally Advanced Non–Small-Cell Lung Cancer: A Secondary Analysis of the NRG Oncology RTOG 0617 Randomized Clinical Trial https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5455690/
Risk of heart disease after radiotherapy DOI: https://doi.org/10.1016/S1470-2045(13)70115-3
Cardiac Toxicity of Thoracic Radiotherapy: Existing Evidence and Future Directions https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7870458/
LAD v15 <10%
Example: IMRT plan delivers LAD v15 of 35% and the proton plan delivers a v15 dose of 8%.
Supporting Data Strength (1 weakest: 5 strongest): 4
Comment: The LAD and SA nodal region appear to currently be the strongest substructures to relate to MACE and OS. As conformality improves and planning awareness improves, there is less correlation between substructures and mean heart dose as noted in the last reference. The chosen metrics is tighter than the first reference and comes from an ASTRO presentation from 2019.
References:
Left Coronary Artery Dose Exposure Predicts Major Adverse Cardiac Events in Coronary Heart Disease Negative Lung Cancer Patients DOI: https://doi.org/10.1016/j.ijrobp.2019.06.470
Comparing Whole Heart Versus Coronary Artery Dosimetry in Predicting the Risk of Cardiac Toxicity Following Breast Radiation Therapy DOI: https://doi.org/10.1016/j.ijrobp.2018.06.091
The Meaningless Meaning of Mean Heart Dose in Mediastinal Lymphoma in the Modern Radiation Therapy Era DOI: https://doi.org/10.1016/j.prro.2019.09.015
The Relationship of Mean Heart Dose and Cardiac Substructure Dose over Evolving Radiation Techniques in Mediastinal Lymphoma
DOI: https://doi.org/10.1016/j.ijrobp.2018.06.228Heart toxicity from breast cancer radiotherapy : Current findings, assessment, and prevention. DOI: 10.1007/s00066-018-1378-z
Liver 30% reduction mean dose
Example: Whole liver IMRT plan delivers mean dose of 15Gy and Proton plan delivers mean dose of 10.5Gy or less.
Supporting Data Strength (1 weakest: 5 strongest): 3
Comment: Data supports liver dose relating to toxicity. Dosimetry metrics are weakly defined and often relate to functional imaging to help in defining risk. Strength of data increased by one based on likelihood of difference having a measurable clinical impact consistent with hepatocellular cancer’s ASTRO Proton Group 1 inclusion.
References:
Protons versus Photons for Unresectable Hepatocellular Carcinoma: Liver Decompensation and Overall Survival DOI: 10.1016/j.ijrobp.2019.01.076
Functional Liver Imaging and Dosimetry to Predict Hepatotoxicity Risk in Cirrhotic Patients With Primary Liver Cancer. DOI: 10.1016/j.ijrobp.2018.08.029
A phase I trial of Proton stereotactic body radiation therapy for liver metastases DOI: 10.21037/jgo.2018.08.17
Dosimetric and Radiobiological Comparison of External Beam Radiotherapy Using Simultaneous Integrated Boost Technique for Esophageal Cancer in Different Location. DOI: 10.3389/fonc.2019.00674
Small Bowel V15: 30% reduction (defined as small bowel within a 5cm distance of the PTV)
Example: Small Bowel volume at 15 Gy is 90cc with IMRT and 45 cc with proton therapy.
Supporting Data Strength (1 weakest: 5 strongest): 4
Comment: Two randomized prospective trials have demonstrated a reduction in bowel symptoms moving from 3D to IMRT (PARCER and RTOG 1203). This is paired with validation data for pelvis. Strength is decreased by 1 as all data is from pelvis with much less clarity in the upper abdomen.
References:
Patient-Reported Toxicity During Pelvic Intensity-Modulated Radiation Therapy: NRG Oncology–RTOG 1203 DOI: 10.1200/JCO.2017.77.4273
Late Toxicity After Adjuvant Conventional Radiation Versus Image-Guided Intensity-Modulated Radiotherapy for Cervical Cancer (PARCER): A Randomized Controlled Trial DOI: 10.1200/JCO.20.02530
The Dose–Volume Relationship of Small Bowel Irradiation and Acute Grade 3 Diarrhea During Chemoradiotherapy for Rectal Cancer DOI: https://doi.org/10.1016/j.ijrobp.2007.06.066
Current and emerging radiotherapy strategies for pancreatic adenocarcinoma: stereotactic, intensity modulated and particle radiotherapy DOI: 10.21037/apc.2018.07.03
Intensity-modulated whole pelvic radiation therapy in patients with gynecologic malignancies DOI: 10.1016/s0360-3016(00)00771-9
Rectum V50; 20% reduction
Example: Rectal DVH is 55% for IMRT and is 33% with proton therapy.
Supporting Data Strength (1 weakest: 5 strongest): 3
Comment: Most data derived from prostate cancer. Potentially more consistency at higher doses but v50 chosen based on patient mix for concurrent pelvic treatment. Clear risk for diarrhea or bleeding with increasing dose. Strength decreased based on lower dose in this patient population.
References:
Radiation dose-volume effects in radiation-induced rectal injury DOI: 10.1016/j.ijrobp.2009.03.078
Use of normal tissue complication probability models in the clinic DOI: 10.1016/j.ijrobp.2009.07.1754
Complications from radiotherapy dose escalation in prostate cancer: preliminary results of a randomized trial
DOI: 10.1016/s0360-3016(00)00700-8
Bone Marrow v20: 40% cc reduction (defined as total pelvic bone)
Example: Bone marrow volume at 40 Gy is 800cc with IMRT and 475 cc with proton therapy.
Supporting Data Strength (1 weakest: 5 strongest): 2
Comment: Retrospective data demonstrates differences in hematologic toxicity based on volume of bone marrow / pelvic bone treated. Articles included have great dosimetric comparisons between IMRT and proton therapy for patients with pelvic disease. Lower strength due to lack of consistent definitions of OAR volume especially for sites above the pelvis.
References:
Correlation between pelvic bone marrow radiation dose and acute hematological toxicity in cervical cancer patients treated with concurrent chemoradiation
DOI: 10.2147/CMAR.S195989Hematologic Toxicity on RTOG 0418: A Phase II Study of Postoperative IMRT for Gynecologic Cancer DOI: 10.1016/j.ijrobp.2013.01.017
Protons offer reduced bone marrow, small bowel, and urinary bladder exposure for patients receiving neoadjuvant radiotherapy for resectable rectal cancer DOI: 10.3978/j.issn.2078-6891.2013.041
Dosimetric Comparison of Intensity Modulated Proton Therapy and Volumetric-Modulated Arc Therapy in Anal Cancer Patients and the Ability to Spare Bone Marrow DOI: 10.14338/IJPT-17-00017
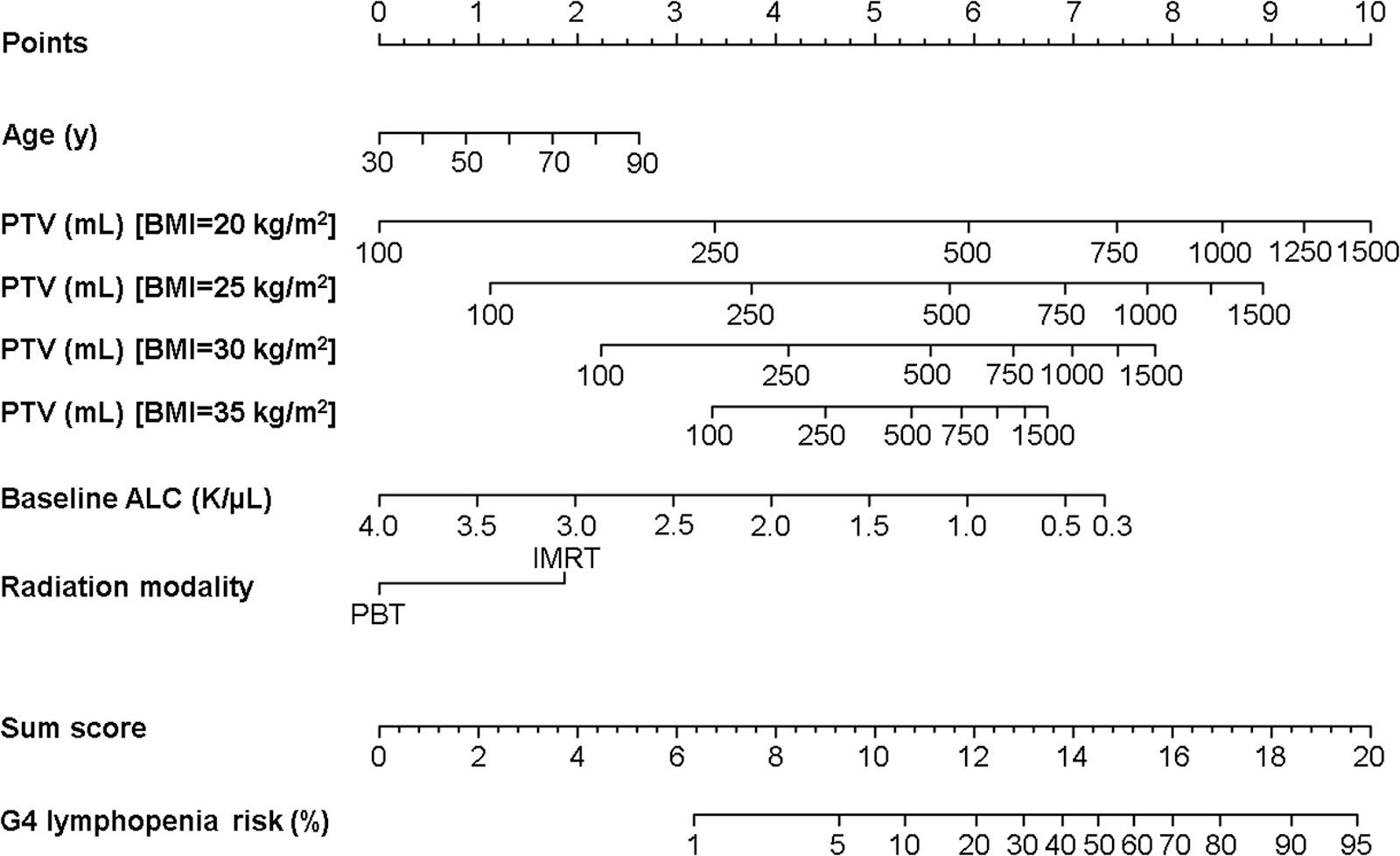
Immune System: 1 nomogram risk group reduction. Breakpoints for Validated Nomogram are: Low<12, Low-Inter 12-13, High-Inter 13-15, High >15
Example: Immune system: Nomogram predicts High risk with IMRT and High-intermediate with proton therapy.
Supporting Data Strength (1 weakest: 5 strongest): 4
Comment: This metric is based upon the EDIC and ERDIC work evaluating radiation’s role in lymphopenia. Data supports lymphopenia risk and radiation dose to the immune system with progression free and overall survival and has been validated. In the chest / thorax, this would be a strength of 5 but due to lack of clear data beyond the chest, it is rated as a 4.
References:
Prediction of Severe Lymphopenia During Chemoradiation Therapy for Esophageal Cancer: Development and Validation of a Pretreatment Nomogram. DOI: https://doi.org/10.1016/j.prro.2019.07.010
Impact of Radiation Dose to the Host Immune System on Tumor Control and Survival for Stage III Non-Small Cell Lung Cancer Treated with Definitive Radiation Therapy. https://doi.org/10.1016/j.ijrobp.2019.05.064
Higher Radiation Dose to Immune System is Correlated With Poorer Survival in Patients With Stage III Non–small Cell Lung Cancer: A Secondary Study of a Phase 3 Cooperative Group Trial (NRG Oncology RTOG 0617) DOI: https://doi.org/10.1016/j.ijrobp.2017.06.351
The Etiology of Treatment-related Lymphopenia in Patients with Malignant Gliomas: Modeling Radiation Dose to Circulating Lymphocytes Explains Clinical Observations and Suggests Methods of Modifying the Impact of Radiation on Immune Cells. DOI: 10.3109/07357907.2012.762780
Radiotherapy-Related Lymphopenia Affects Overall Survival in Patients With Lung Cancer DOI: https://doi.org/10.1016/j.jtho.2020.06.008
APPENDIX: Lymphopenia Nomogram
www.protons101.com, home of the original Protons 101 website.
Content for the Protons101 blog written by Mark Storey MD.
Subscribe to Protons 101
A Substack dedicated to Radiation Oncology with an emphasis on technology, business, and the tremendous value we represent in the field of oncology. Technical content in a less formal setting. All the cool kids are here - join us!
If you aren't already collaborating with Jeff Ryckman and the radoncreview.org folks, you should! Similar efforts. Lots of work!